
Hughes 369HS

Photo copyright MD Helicopters - used with permission
Private Pilot, N9116F
Talladega, Alabama
July 12, 1993
On July 12, 1993, a private helicopter, a Hughes 369HS, crashed while attempting to land in the infield of the Talladega Superspeedway after a 60-mile flight. The landing zone was described as a small, fence-enclosed parking lot. The landing area, which included a media center building, was surrounded on all sides with obstructions, including tall chain-link fences and power lines. Other landing zone hazards included adverse wind conditions which resulted in a downwind landing. The pilot of the helicopter was killed, and the passenger was treated for serious injuries.
The National Transportation Safety Board (NTSB) determined the probable cause of this accident to be the pilot's poor in-flight decision to land downwind in a confined area that was surrounded by high obstructions, and his failure to properly compensate for the tailwind condition. A factor related to the accident was the pilot's lack of experience in the type of aircraft.
NTSB Report Number: ATL93FA127

Photo copyright MD Helicopters - used with permission
History of Flight
On July 12, 1993, a private helicopter, a Hughes 369HS, departed Birmingham, AL about 1415 CDT en route to Talladega Superspeedway. After a 60-mile flight, the pilot attempted a landing in adverse conditions that included environmental and physical obstacles. Upon approach to the speedway, he selected a landing area that was surrounded on all sides by tall fences, power lines, and a building. In addition, the approach heading, and the wind conditions resulted in an attempted landing with a downwind component.
Prior to the crash, witnesses to the accident stated that the helicopter approached the intended landing zone from the south at an altitude of about 50 feet. Once the helicopter was over the landing area, the helicopter began to descend slowly from an approximate height of 50 feet in a hover to approximately one foot above the intended landing zone. At this point, the helicopter began to oscillate from side to side and then climbed to an altitude of approximately 25 feet. After reaching this height, the helicopter began to rotate in a counterclockwise direction. The helicopter then banked sharply to the left and impacted the ground and a 10-foot fence. The pilot of the helicopter was killed. The passenger was treated and released with a broken collarbone and fractured ribs.

Photo copyright MD Helicopters - used with permission
Aircraft Information
The accident aircraft was a Hughes Model 369HS (Normal Category Helicopter) Part 27 which received FAA certification on January 3, 1969. The serial number of the accident aircraft was 0396S and the year of manufacture was 1972. The Hughes 369HS has a 5-bladed, rigid rotor system with an Allison 250-C20 engine (278 horsepower rating). This aircraft is a highly maneuverable helicopter as compared to the R-22, the aircraft used during the accident pilot's initial rotorcraft training. The less complex R-22 has a reciprocating engine, de-rated to provide 131 horsepower, with a teetering, 2-blade rotor system.
According to the NTSB report, the pilot occupied the left seat at the time of the accident. The non-rated passenger was in the right seat where dual controls were installed. Typically, helicopters are operated with the pilot in command sitting in the right seat; however, the 369HS is certified for left-seat pilot in command.
Rotorcraft Flight Manual (RFM)
Due to the aggressive, highly responsive handling characteristics of the Hughes 369HS, the Rotorcraft Flight Manual (RFM) discusses these traits in Section IV, Normal Procedures. The emphasis in paragraphs 4-8 highlights the issues involved with low-speed maneuvering. It provides information for avoiding maneuvers that exceed the thrust capability of the tail rotor. These conditions in which thrust limits may be approached include, high density altitude, high gross weight, rapid pedal turns, and downwind conditions. The RFM also mentions avoiding any maneuver that requires full pedal, extreme aircraft attitudes, and maneuvers at low speeds.
The RFM states that controllability during downwind hovering, sideward flight, and rearward flight conditions have been demonstrated to be adequate in winds up to 20 knots. FAA certification of this aircraft included flight testing and did not mandate that the crosswind or tail wind limits be included in the RFM.
Accident Site
Due to evidence of aircraft loss of control, the investigation required a detailed examination of the main rotor and two tail rotor driveshaft systems and the two-tail rotor pedal stems. The continuity of the flight controls was confirmed throughout the helicopter. Dual controls were installed in the aircraft at the time of the accident. All non-destructive inspections of the concerned components revealed fractures consistent with overstress or due to the sudden stoppage of the main rotor system. The two-tail rotor pedal stems were examined, and no evidence supported any failures that would lead to subsequent loss of control of the helicopter.

View Larger
Landing Zone Information
The specifications of the landing site were 168 feet long by 105 feet wide and it was surrounded on all four sides by tall fences and power lines. Helicopters are designed to accomplish vertical take-offs and landings. The landing zone was within the infield of the speedway and it was also located adjacent to Talladega Municipal Airport.
Landing Selection Decision-making
According to the FAA's Helicopter Flying Handbook, each pilot should perform a risk assessment prior to landing zone selection. This determination must include not exceeding the capabilities of the aircraft and pilot. Helicopter pilots should perform both high- and low-reconnaissance orbits of the intended landing zone to identify suitability of the landing zone, approach and departure paths, prevailing wind conditions and obstacles. The NTSB report indicated that the helicopter instructor did not conduct any downwind landing training with the accident pilot. It is unknown if, at the time of the accident, the racetrack had a helipad for helicopter air ambulance aircraft or was equipped with a windsock, visible to the pilot, within the immediate vicinity.
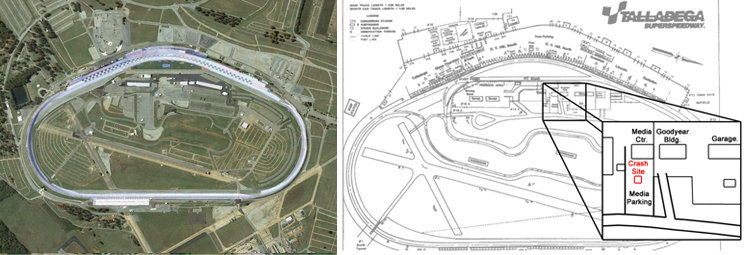
Diagram of Talladega Superspeedway showing location of crash site (right)
View Larger
Meteorological Information
Per the NTSB report, visual meteorological conditions (VMC) existed at the time of the accident and the pilot had not filed a flight plan. It is unknown if the accident pilot had obtained a weather briefing prior to the flight. Weather conditions at the landing zone were reported by witnesses to have wind conditions blowing from the south. The weather facility cited in the NTSB report was Anniston Regional Airport (ANB), which was 12 nautical miles east of the accident site. The reported weather conditions at 1450 CDT were reported as scattered clouds at 4,000 feet AGL with a temperature of 90º F and a/dew point of 72º, F with visibility of six miles and the winds were from 130º at five knots. This weather report was issued five minutes prior to the time of the accident.
In general aviation, remote landing zones often do not have wind indicators; however, in an environment such as Talladega Superspeedway there were many flags and banners to assist a pilot in determining landing wind conditions.
Pilot Experience
The accident pilot had accumulated approximately 1,073 hours of total flight time in all aircraft. He received his helicopter rating in July 1992, approximately one year prior to the fatal accident, and he had completed approximately 54 hours of flight time in helicopters. He had flown approximately nine hours in the Hughes 369HS and accumulated the remaining flight time during training for his helicopter rating in a Robinson R-22. His flight experience in all aircraft included 963 hours as pilot in command and 31 hours in the last 30 days.
The accident pilot received dual flight instruction in the accident aircraft totaling 2.8 hours over two training sessions in the previous month. The flight instructor provided a statement that during the flight training in the Hughes 369HS, the following maneuvers were practiced: take-off and landings, auto-rotations to power recovery, and quick stop procedures. He indicated that at no time during the training had they practiced downwind landings. After the completion of the last training session, the accident pilot informed the flight instructor that he intended to fly the helicopter to his private residence and it would remain there until after the Talladega race. The accident pilot was to schedule an additional training flight with the flight instructor at a later date to complete an endorsement in the Hughes helicopter prior to conducting any flights with passengers.
The pilot's limited time in type and the high-performance characteristics of the new helicopter indicated a need for additional training. Insurance companies often stipulated additional flight requirements on pilots who fly under their policies. The NTSB docket included an insurance company quote to the accident pilot that not only mandated the completion of 25 hours of flight training in the Hughes 369HS prior to solo flight but also 25 hours of solo flight prior to carrying any passengers.
Make and Model Transition Training
Pilot experience in specific make/model is essential to the safe operation of aircraft in general aviation. The successful training and subsequent checkout on additional aircraft is critical for the professional development of pilots. Also the training should be provided by a trained and qualified pilot who has extensive knowledge and experience in the specific make/model. The training should include all aspects of safe operations and emergency procedures. In the instance of this accident, the pilot received a rotorcraft certificate add-on rating within the past year; this required increased emphasis on ensuring a full and complete check out in the new make/model.
Helicopter Design and Aerodynamics
The Hughes 369HS has a tail rotor design that features a tail rotor blade advancing downward or away from the main rotor blade. Often this design creates less than optimal directional-control characteristics over those with tail rotor blades advancing upwards and reduces the tail rotor's effectiveness. Later models of the Hughes 369 incorporated different designs to the tail rotor blade direction, tail rotor blades, and vertical fin configurations.
FAA CFR Part 27.143 Controllability and Maneuverability requires that the aircraft must be safely controllable and maneuverable in all phases of flight in wind velocities from zero to at least 17 knots from all azimuths. Additionally, it must be shown that the rotorcraft can be operated without loss of control on or near the ground in any maneuver appropriate to the type of aircraft.
Tail Rotor Effectiveness
Helicopter design requires an anti-torque system to counteract main rotor torque and prevent spinning once the helicopter lifts off the ground. In addition to design limitations, environmental forces, such as a tailwind, can overwhelm any aircraft, especially the inherently unstable helicopter. The tail rotor is certified for normal flight conditions. However, there are prevailing wind conditions that can overwhelm the tail rotor, leading to loss of tail rotor effectiveness.
Loss of Tail Rotor Effectiveness (LTE)
While the accident report does not specifically state that LTE was a cause of this accident, the NTSB points out that attempting to land in a tailwind was a causal factor. LTE is a common concern for helicopter pilots, and is defined as an uncommanded, rapid yaw towards the advancing blade, which does not subside of its own accord. LTE is a condition created by wind factors. It is caused by an aerodynamic interaction between the main rotor and tail rotor and is not caused from a mechanical failure or maintenance malfunction. It may occur in varying degrees in all single main rotor helicopters at airspeeds less than 30 knots.
The design of main and tail rotor blades and the tail boom assembly can affect the characteristics and susceptibility of LTE but will not eliminate the phenomenon entirely. Loss of the aircraft can occur if the pilot does not initiate recovery from LTE.
The FAA Helicopter Flying Handbook provides generic recovery procedures for LTE. In some helicopter models, a pilot may find himself outside the performance envelope where power required exceeds the power available. Thus, a pilot may be expecting more performance from the aircraft than is possible.
Types of LTE
There are three general forms of LTE as described in the Helicopter Flying Handbook: main rotor disc vortex interference, vortex ring state, and weather cocking.
Main Rotor Disc Vortex Interference
Relative wind within ±15° of the 10 o'clock position, generating vortices that can blow directly into the tail rotor. This is dictated by the characteristics of the helicopter's aerodynamics of tail boom position, tail rotor size and position relative to the main rotor and vertical stabilizer, size, and shape.
Tail Rotor Vortex Ring State
Tail rotor vortex ring state involves winds from 210° to 330°. Winds within this region result in the development of the vortex ring state of the tail rotor.
Weathercock Stability
Weather cocking involves tailwinds from 120° to 240°, such as left crosswinds, causing high pilot workload.
In this accident, investigators concluded that the pilot's downwind landing subjected him to tailwinds associated with weather cocking, where the helicopter attempts to weathervane its nose into the relative wind. Unless the pilot makes an opposing pedal input, the helicopter starts a slow, uncommanded turn either to the right or left, depending upon the wind direction and main rotor blade rotation. If the pilot allows a yaw rate to develop and the tail of the helicopter moves into this region, the yaw rate accelerates rapidly. In order to avoid the onset of LTE in a tailwind condition, it is imperative to maintain positive control of the yaw rate and complete a recovery maneuver immediately to prevent loss of control.
For additional information on Downwind landings, see the attached article Pushing the Limits.
For additional information on LTE, see the Helicopter Flying Handbook, FAA-H-8083-21A.
The Rotorcraft Flight Manual for the MD 369HS does not specifically address downwind landings; however, there is a note which states "Controllability during downwind hovering, sideward and rearward flight has been demonstrated to be adequate in winds up to 20 knots."
The Rotorcraft Flight Manual is available at the following link: Rotorcraft Flight Manual - MDHI 500 Helicopters.

View Larger
Landing Performance Considerations
Landing a helicopter requires consideration of location and surrounding obstacles in addition to environmental conditions. A high and low reconnaissance (recon) is recommended prior to landing in a confined-area landing zone or unfamiliar site. During a high recon, it is recommended that three orbits be conducted to identify hazards, direction and speed of wind, location of a touchdown point, suitability of landing area, approach and departure headings, and location of obstacles. The high recon should be performed at an altitude of at least 500 feet AGL at a forward speed of 60 knots. After completing the high recon, the pilot should transition to a low recon and complete a similar assessment. The low recon should be performed at 100 - 200 feet. During the reconnaissance, consideration must also be given to the helicopter's maneuverability and performance during landing and a recovery plan should be devised in the event of encountering LTE.
Survivability
The debate on whether or not to use helmets in helicopter operations has been ongoing since early flight, despite studies that prove their effectiveness in survivable accidents. A 1991 study by the U.S. Army supported the effectiveness of the SPH-4 flight helmet in reducing severe head injuries sustained during helicopter accidents. The analysis that was restricted to severe (Class A) accidents that were at least partially survivable, proved that occupants not wearing a protective helmet were significantly more likely to sustain severe and fatal head injuries than were occupants wearing the SPH-4. The U.S. Army found the risk of fatal head injury to be 6.3 times greater for those not wearing helmets.
A 2013 FAA collaborative project on post-crash fire and blunt force fatal injuries from 97 civil helicopter accidents revealed that blunt force trauma (BFT) was the cause of death in 92% of all fatal rotorcraft accidents. Of the BFT injuries, 50% were to the skull, while 65% included brain injuries. Both of these studies indicate that use of helmets in helicopter operations is effective and increases the chance of survival.
Conclusion
According to investigators, the accident pilot experienced a loss of tail rotor effectiveness. His lack of experience in the make/model of the aircraft, along with obstacles in a confined area and a tailwind in the final approach to the landing zone, created an LTE condition. The pilot's limited experience, lack of reconnaissance procedures, and no recovery plan were germane in his decision to land in this confined area. Once he made the decision to land in this area he encountered LTE and experienced a loss of control from which he did not recover.
Witness statements described the aircraft path as a single approach to the landing zone from the south. When the aircraft was at an altitude of about 50 feet and over the landing area, the aircraft began a slow decent to approximately one foot above the terrain. It was during this critical phase of flight that the aircraft began to oscillate from side to side and then climbed to an altitude of approximately 25 feet. After reaching this new height, the aircraft began to rotate in a counterclockwise direction.
According to the FAA Helicopter Flying Handbook, if rotation cannot be stopped and the close proximity to the ground does not allow any forward cyclic input, and ground contact is imminent, an autorotation should be attempted. The accident pilot did not attempt an autorotation and, with the aircraft out of control, the helicopter banked sharply to the left and impacted terrain and a ten-foot fence adjacent to the originally intended landing site. Investigators determined that had the pilot immediately lowered the collective when the aircraft was one foot above the terrain and the helicopter was experiencing the onset of LTE, the aircraft would have touched down.
Per the NTSB report, the pilot and passenger were not wearing helmets. A credible news source reported the pilot sustained head injuries and later died. The passenger was treated for a broken collarbone and fractured rib. No autopsy or toxicology was performed on the accident pilot.
Memorial
Following the pilot's death, the family elected to donate his organs to support the needs of critically ill patients. In addition, the R. K. Allen Oil Company funded the development of a Talladega-Texaco Walk of Fame in Talladega, AL, a park to memorialize the pilot and celebrate various accomplished NASCAR drivers.
The NTSB determined the probable cause of this accident to be the pilot's poor in-flight decision to land downwind in a confined area that was surrounded by high obstructions, and his failure to properly compensate for the tailwind condition. A factor related to the accident was the pilot's lack of experience in the type of aircraft.
Findings: None.
NTSB Report Number: ATL93FA127
FAA 14 CFR Part 27.143, Controllability and maneuverability
Advisory Circular (AC) 90-95, Unanticipated Right Yaw in Helicopters
This advisory circular examines unanticipated right yaw phenomenon, the circumstances under which it may be encountered, how it can be prevented, and how the pilot should react if it is encountered.
As the pilot was not part of an air carrier operation, no organizational factors were identified by the NTSB. The accident pilot purchased a new, high-performance aircraft but had only completed 2.8 hours of instruction. He was authorized to fly the helicopter solo to his home, but he required more instruction prior to further solo or passenger-carrying operations. Additionally, his insurance company issued a quote for a policy that required completion of 25 hours of dual instruction and 25 additional hours of solo flight. Despite his minimal time in the Hughes aircraft, lack of endorsement, along with only 54 hours total helicopter time, he chose to conduct a flight with a passenger and attempted to land in a challenging landing zone.
- Wind conditions that could potentially lead to loss of tail rotor effectiveness
- Hazards associated with landing in confined areas of operations and surrounding obstructions
- The hazards of choosing not to wear personal protective equipment that may reduce injuries
Tail rotors are effective through all ground and flight operations.
- Even relatively light winds, especially those associated with tailwinds, can result in loss of tail rotor effectiveness. The pilot attempted to land in a confined area that had downwind conditions limiting his ability to maintain control of the aircraft.
Pilots conduct reconnaissance to choose a safe landing field.
- The accident pilot did not conduct proper reconnaissance before selecting a landing zone. Instead, he attempted to land the helicopter in a confined area with several high obstacles, a tail wind, and no escape path.
Pilots will make use of available protective equipment such as helmets goggles to reduce the risk of injury.
- The pilot did not use any personal protective equipment. A helmet may have reduced the head trauma he received.
NTSB Safety Alert, SA-062 March 2017
"Be alert for uncommanded yaw so you don't get caught off guard!"
View: NTSB Loss of Tail Rotor Effectiveness (LTE) Safety Alert Video
U.S. Helicopter Safety Team (USHST) Helicopter - Safety Enhancements (H-SE)
- Helicopter Safety Enhancement (H-SE) Number 124:
- Helicopter Safety Enhancement (H-SE) 123-1:
- Helicopter Safety Enhancement (H-SE) 81:
Rotorcraft Life Cycle:
- Operational
Accident Threats:
- Loss of Control - Inflight (LOC-I)
Industries:
- Personal / Private
Accident Common Themes:
- Human Error
- Flawed Assumptions
Human Error
The accident pilot failed to maintain aircraft control in a highly demanding landing in adverse conditions (e.g., tailwind) and confined area. Investigators concluded these factors exceeded the pilot's capability and experience in the Hughes 369HS.

NTSB Identification: ERA12MA005
Aircraft: Bell 206B, registration: N63Q
Accident Occurred: October 04, 2011, in New York, NT
Injuries: 2 Fatal, 1 Serious, 2 None
Analysis
The purpose of the flight was for the pilot to take friends on a sightseeing flight around New York City, departing from the East 34th Street Heliport (6N5). The pilot did not conduct a safety briefing or mention life vests available on board the helicopter, complete performance planning, or perform weight-and-balance calculations before takeoff.
The helicopter departed 6N5 in a rearward hover and transitioned over the shoreline from an in-ground-effect condition to an out-of-ground-effect (OGE) condition while climbing to about 60 feet above the water. As the pilot completed a pedal turn into the wind, the helicopter yawed, and what was likely the low rotor rpm audio warning sounded. After the pilot increased collective pitch, the helicopter entered an uncommanded right yaw that accelerated into a spin around the main rotor mast that could not be corrected by application of full left pedal. The pilot lost control of the aircraft and subsequently crashed into the East River.
Probable Cause and Findings
The NTSB determined the probable cause of this accident to be the pilot's failure to anticipate and correct for conditions (high gross weight, low indicated airspeed, and a right downwind turn) conducive to loss of tail rotor effectiveness (LTE), which resulted in LTE and an uncontrolled spin. Contributing to the accident was the pilot's inadequate preflight planning, which resulted in the helicopter being in excess of its maximum allowable gross weight at takeoff.

NTSB Identification: CEN13FA205
Aircraft: Hughes OH-6A, registration: N910WC
Accident Occurred: March 26, 2013, in Caddo, TX
Injuries: 1 Fatal, 1 Minor
Analysis
The helicopter approached an open field, adjacent to a stock pond, where it had landed earlier in the day. The pilot stated that he looked for smoke or dust to establish the velocity and direction of the wind before landing, but that he did not observe any. As the pilot established a hover about 3 to 4 feet above the ground, he turned the helicopter east-southeast. Subsequently, the helicopter started to spin (onset LTE), and the pilot was unable to regain control. The helicopter impacted the stock pond on the passenger side and immediately sank. The pilot escaped from the helicopter; however, the passenger was unable to exit the helicopter due to a head injury.
Probable Cause and Findings
The NTSB determined the probable cause of this accident to be the pilot's failure to maintain control of the helicopter during landing.

NTSB Identification: WPR13FA343
Aircraft: Robinson R44II, registration: N25WH
Accident Occurred: July 27, 2013, in Thompson Falls, MT
Injuries: 1 Fatal, 1 Serious, 1 Minor
Analysis
The helicopter was following a line of utility poles for an aerial survey flight. Surviving passengers reported the helicopter was flying straight and level before it began to spin. Additionally, the helicopter, as a result of a tailwind, began to rotate in a clockwise direction and experienced LTE just before impact. It was reported that the low rotor rpm warning horn sounded. The helicopter impacted heavily forested terrain in a steep nose-down, right-bank attitude.
Probable Cause and Findings
The NTSB determined the probable cause of this accident to be the pilot's failure to maintain helicopter control while operating in conditions conducive to a loss of tail rotor effectiveness.
Technical Related Lessons
Loss of Tail Rotor Effectiveness (LTE) is a critical, low-speed aerodynamic flight characteristic which could result in an uncommanded rapid yaw rate which does not subside of its own accord. If not corrected, LTE could result in the loss of aircraft control. (Threat Category: Loss of Control - Inflight (LOC-I))
- LTE is caused by an aerodynamic interaction between the main rotor and tail rotor and not from a mechanical failure. LTE may occur in varying degrees in all single, main rotor helicopters at airspeeds less than 30 knots. Downwind landings should be avoided due to the potential of exceeding tail rotor authority
- Limitations on the 369HS are more restrictive, as this aircraft's handbook documents a demonstrated capability of only 20 knots
- If a sudden unanticipated yaw occurs, the Helicopter Flying Handbook recommends the following recovery technique:
- Apply forward cyclic control to increase speed
- If altitude permits, reduce power
- As recovery is affected, adjust controls for normal forward flight
- Always plan a recovery path, especially when terminating to an out-of-ground effect hover and immediately take action if an uncommanded yaw occurs
- Avoid downwind landings due to the potential of exceeding tail rotor authority
- The HS369 Rotorcraft Flight Manual (RFM) includes the following comments in the Section 4-8. LOW SPEED MANEUVERING:
- Avoid maneuvers that exceed thrust capability of the tail rotor
- NOTE: Conditions where thrust limits may be approached are: High density altitude, high gross weight, rapid pedal turns, and placing the helicopter in a downwind condition
- Avoid any maneuver that requires full pedal
- Avoid extreme aircraft attitudes and maneuvers at low speeds
- Controllability during downwind hovering, sideward flight, and rearward flight has been demonstrated to be adequate in winds up to 20 knots
Common Theme Related Lessons
Pilots should select a suitable landing zone, considering their experience and the capabilities of the aircraft, especially in tailwind conditions. (Common Theme: Human Error).
- Pilots should evaluate wind conditions to ensure they do not inadvertently put the aircraft downwind into a tailwind condition that could lead to LTE
- This accident highlights the importance of training that should include all aspects of safe operations and emergency procedures as well as the necessary experience to address environmental factors
Injury to helicopter pilots can be reduced or avoided by use of appropriate personal protective equipment (PPE), such as helmets, flight boots, and flight gloves. (Common Theme: Flawed Assumption).
- The accident pilot was not wearing a helmet and sustained fatal head injuries
- A 2013 FAA collaborative project on post-crash fire and blunt force fatal injuries from 97 civil helicopter accidents revealed that blunt force trauma (BFT) was the cause of death in 92% of all fatal rotorcraft accidents. Of the BFT injuries, 50% were to the skull, while 65% included brain injuries