
Boeing 727-95

Photo copyright Bob Polaneczky - used with permission
American Airlines Flight 625, N1963
St. Thomas, Virgin Islands
April 27, 1976
At 1510 local time, American Airlines Flight 625, a Boeing Model 727-95, was landing at Harry S. Truman Airport on St. Thomas Island of the U.S. Virgin Islands. During the landing, the airplane floated and touched down long, well outside the required touchdown zone, on this very short runway. The captain, thinking he did not have enough runway to stop, attempted a go-around. Believing the engines were not responding rapidly enough for a successful go-around, he aborted the go-around and attempted to stop. The aircraft skidded off the end of the runway, crashed through the airport boundary fence, went over a road, and came to rest against a gas station. Thirty seven of the 88 passengers and crew aboard were killed. One person on the ground was seriously injured.
The National Transportation Safety Board (NTSB) concluded that the probable cause was the captain's actions and his judgment in initiating a go-around with insufficient runway remaining after a long touchdown. The long touchdown was attributed to a deviation from prescribed landing techniques and an encounter with an adverse wind condition, common at the airport.
Contributing factors noted were the non-availability of go-around performance information that may have been a factor in his decision to attempt the go-around. The deviations noted above included:
- The pilot's decision to not fly the approach and landing with the flaps in the proper, maximum deflection as prescribed by the airline's procedures for this airport with the reported wind conditions. The captain decided to fly the approach at Flaps 30 degrees, rather than the prescribed 40-degree setting. The 30-degree flap setting requires a higher approach speed and results in a longer landing distance.
- The deviation from company procedures by not executing a go-around once he had floated past the company-designated required touchdown zone.
History of Flight

American Airlines (AAL) Flight 625 was a scheduled flight from Providence, Rhode Island to Charlotte Amalie, St. Thomas, U.S. Virgin Islands, Harry S. Truman Airport, with a planned intermediate stop at New York. Since the accident, the airport has been renamed Cyril E. King airport. There were 81 passengers and 7 crewmembers (three flight crew and four cabin crew) on board the aircraft.
On arrival in the St. Thomas vicinity, the flight was cleared to fly a visual approach to runway 09. This was the only runway on which American Airlines allowed 727 landings at St. Thomas. This was directed by a 1971 company letter 1971 company letter to Caribbean flight crews and American Airlines Operations Bulletin FM C-7. This was due to the runway being very short (4,650'), and because runway 09 was the only runway with an Instrument Landing System (ILS) approach.
The approach from over the water was flown manually, aided by ILS guidance. The figure below is a photograph of the airport near the time of the accident.
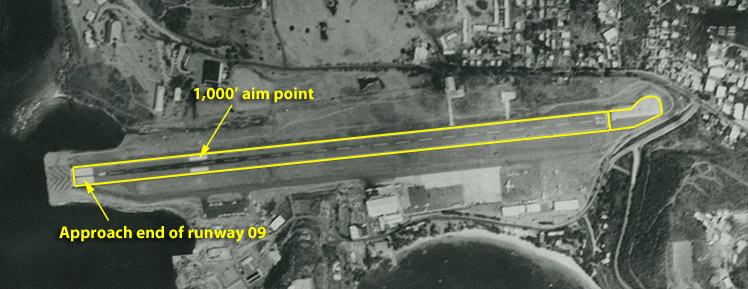
Photo courtesy of U.S. Virgin Islands Port Authority
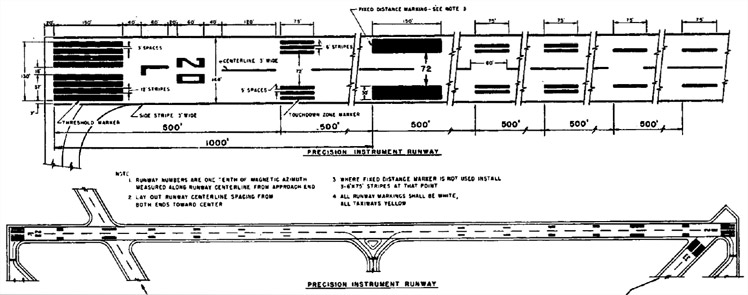
Note the wide white stripes at the approach end of runway 09 (left side of photo) and at the 1,000 foot aim point, indicating this runway had a precision approach (ILS). The runway was 4,650 feet long with 515 feet of overrun (lighter area at right end) which would support an aircraft during landing roll, but was not allowed to be used for landing distance calculations. During a normal approach, it was expected that the ILS would guide the airplane towards the 1,000' aim point, and the airplane would flare and touch down within the next 1,000 feet.
At the time of the accident, the weather was reported as VFR, with scattered clouds at 2,500 feet, overcast at 12,000 feet, and the winds were 12 knots from 120 degrees with no gusts reported. This resulted in a 10-knot headwind component and a six knot crosswind from the right. With these winds, per American Airlines Operations Bulletin FM C-7, the captain would normally have flown the approach using a 40-degree flap setting (Flaps 40). However, in post-accident interviews, the captain said when he heard the winds were from the southeast, from his experience he assumed they would be gusty, and the Ops Bulletin allowed use of Flaps 30 "with strong or gusty winds." The captain ultimately chose to fly the approach using Flaps 30. Use of Flaps 30 increased the approach speed by four knots and the calculated landing distance by 300 feet. However, this was still well within the available runway.
Investigators determined that the pilot flew a stabilized approach with the aircraft on speed, and only a "shade below" glideslope at the approach end of the runway (corroborated by aircraft waiting to takeoff). During the landing flare, a wind gust rolled the aircraft slightly. During the correction, the aircraft "floated" down the runway until the second officer called that they were still high. At this point, per company guidance described above, a go-around should have been initiated. Instead, the captain forced the airplane onto the runway approximately 2,800' from the approach end (as indicated by tire marks), nearly 1,500 feet beyond the designated touchdown zone. This left 1,858 feet of runway and 500 feet of overrun remaining.
The investigation described the events after touchdown as follows. The captain decided that he could not stop the aircraft on the remaining runway, and he called for a go-around. He placed the throttles "straight up" per company procedure, but he did not believe that the engines were responding rapidly enough, so he shoved them full forward. He did not call for flaps to be moved to the go-around position (25 degrees). The first officer asked the pilot if he wanted Flaps 25, and the pilot called for Flaps 15, a takeoff flap setting. This was also not per procedure, so the first officer moved the flaps to the proper 25-degree go-around position. The captain then felt they were "not going anywhere" and realized they would not be able to do a successful go-around. He moved the throttles to idle and applied full brakes with 1,215 feet of hard surface remaining (runway and over-run). The speed brakes were not deployed, but the captain, in post-accident interviews, felt he may have gotten the engines into reverse thrust by the time the aircraft left the runway. Post-crash inspection showed both reversers were only partially deployed.
The airplane slid approximately 525 feet past the end of the overrun, clipping an antenna, going through the airport boundary fence, crossing a road, and coming to rest against a gas station.
Below is a simplified diagram of the runway with key points noted from the accident report. This illustrates how far past the desired touchdown area the airplane actually touched down, how much runway was used while attempting a go-around, and, finally, how little runway remained when the decision to stop was made.
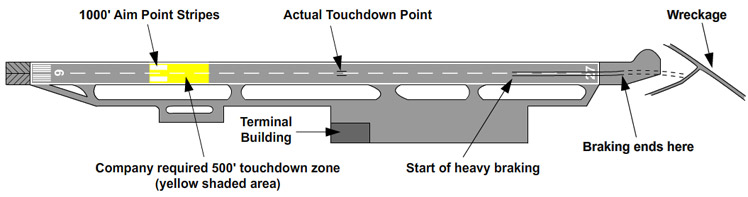
View original diagram from the accident report
For a visual description of the accident sequence, view an animation of the accident event with detailed narration below:
View a second animation in real time of accident including the flight deck communications below:
Runway Situational Awareness
The investigators determined that in this accident the pilot's awareness of the aircraft's position relative to the touchdown zone, and to the end of the runway, were paramount. In various company memos it was stressed that due to the short runway length the aircraft needed to touch down within 500 feet of the touchdown aim point, thus 1,000 - 1,500 feet from the threshold.
Touchdown zone
The investigation determined that the aircraft encountered turbulence very near the flare point, requiring the captain to focus on leveling the wings. Subsequently, the airplane floated well beyond the touchdown zone. The touchdown zone was 500 feet long, and at the selected approach speed, the airplane would have transited this zone in about 2.5 seconds. The airplane floated for approximately seven seconds. The investigation focused on why neither the first officer nor the flight engineer alerted the pilot that he had exceeded the touchdown zone and should have initiated a go-around. In fact, the investigation noted that the first officer commented, "You're still high Art" after seven seconds, urging the pilot to land.
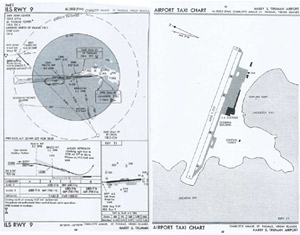
Right, airport map chart - View Larger
727 Landing Performance
The 727 flap system was designed to minimize landing distance, allowing the airplane to access airports with short runways. On a typical wing/flap system, as the flap angle is increased the lift and drag are also increased. However, on the 727, Flaps 40 was a rather large deflection, and the main effect was an increase in drag with a lesser corresponding increase in lift. The large drag increase required higher thrust during the approach, and also shortened the landing distance by a noticeable amount (~250 feet) compared to the Flaps 30 position. However, the general consensus among 727 operational pilots at the time was that it was easier to make a smooth landing at Flaps 30 than at Flaps 40. Thus, on long runways where landing distance was not really a factor, Flaps 30 became the customary landing flap choice. The investigators determined that this may have been a contributing factor to the pilot's decision to use Flaps 30 instead of the American Airlines Operations Bulletin recommendation of Flaps 40 at this airport.
Airplane Stopping Performance
Airplane landing distance is determined during certification flight testing of the aircraft. Performance landings are conducted with maximum braking on smooth dry runways at a range of speeds, weights, and flap settings. From this, the "air" distance (the distance covered over the ground from a 50-foot altitude to touchdown) is derived. Deceleration devices, such as speed brakes, are used per the manufacturer's recommended procedure. No performance credit was allowed for thrust reversers. At the time of the 727 certification, thrust reversers were not considered to be sufficiently reliable, compared to the brakes and other deceleration devices, and it was considered conservative to disregard their performance contribution. Braking tests were conducted at increasing weights and speeds (energies), up to the maximum demonstrated brake energy, to develop the braking performance model. These data were then used to develop the landing performance charts used by the airlines to operate the aircraft.
Landing distances include time delays for braking initiation and time to deploy deceleration devices such as speed brakes. It must be noted that per Air Carrier Operations rules in place at the time of the accident, 14 CFR 121.195, "Airplanes: Turbine Engine Powered: Landing limitations: Destination airports", the landing distance in the FAA-approved airplane flight manual must be less than or equal to 60% of the available runway (overrun is not included). This performance factor is a safety margin to allow for operational variations due to wind, runway surface condition (wet or dry), touchdown dispersion, etc.
The investigators analyzed the accident conditions and determined that the aircraft should have been able to stop in approximately 1,730 feet after touchdown. This means that even after the long landing, if the pilot had immediately initiated maximum braking and deployed the speed brakes and thrust reversers, the airplane would have stopped very near the end of the runway. However, according to the investigators, the pilot, when making the final decision to stop, did not apply maximum braking and did not deploy speed brakes or thrust reversers.

Right, photo of east end of St. Thomas Airport. Photo copyright Elliot Epstein - used with permission
Airplane Go-around Performance
The NTSB investigated the go-around performance of the 727. Calculations were done using various engine acceleration times and airspeeds at initiation. Distance from initiation to liftoff varied from 1,912 - 2,448 feet. At an initiating speed of 110 knots on the ground, and a pause at a power setting of 1.4 EPR (per procedure), the distance to liftoff was calculated to be 2,387 feet. Based on these calculations, the investigators concluded that a successful go-around could not have been executed from the point at which it was initiated.
Flight Crew Decision Making
The captain's actions and his decision making became the focus of the NTSB's analysis. The investigation stated that following the turbulence encounter, when the designated touchdown zone had been missed and while the airplane was still in the air, the captain should have made the decision to execute a go-around. Further, having missed that opportunity once having landed, the captain should have lowered the nose, applied maximum braking, and deployed all additional deceleration devices. This action would likely have resulted in a successful stop near the end of the runway, or at the least, a less consequential overrun.
The investigation concluded that the captain's decision making may have been influenced by his lack of knowledge of airplane performance, relative to airplane go-around and stopping performance. In the official accident report, the NTSB stated:
"Thus, while the Safety Board believes that the causal area of this accident involves the captain's actions before and after the touchdown, his lack of substantive information about the aircraft's stop or go around performance capabilities seriously affected his ability to make a proper decision in this situation. The Board is aware that American Airlines' training procedures have been revised to include these performance factors. An Operations Bulletin (FM2 C-13) was issued on August 16, 1976, and placed in the Flight Manual. The bulletin states that any decision to go-around at St. Thomas should be made and initiated no later than the 1,000-foot touchdown markers. This bulletin continues with the following company policy:
"Go-around shall not be attempted after the aircraft has touched down on the runway, and the landing should be continued to a stop -- recognizing the full stopping capabilities of the 727 with spoilers, main and nose gear brakes."
Visual Re-creation

In 2012 a 737 flight simulator exercise was performed by FAA Flight Test personnel in order to provide a visual representation of what the pilots may have seen during the accident. This exercise was intended to enhance the knowledge of the two key decision points identified by the accident investigators (the airborne go-around and post touchdown stopping), and to provide a sense for the rapidity with which events occurred. These re-creations are for visual informational purposes only and are in no way completely accurate in recreating the aircraft performance.
The 737 is similar in weight and size to the 727, so the operating speeds for landing and visual perspectives are comparable. The simulator's visual presentation was for runway 21 at Portland International Airport. It is 6,000 feet long. Thus, to simulate the approach to St. Thomas, the pilot used an aim point of 4,100 feet from the end of the runway. Several different scenarios were examined. View the videos below:
The actual accident scenario as best as could be duplicated visually.
The landing if the pilot would have performed a full stop, even after touching down long, as was the case in the accident. In this simulation, the airplane stopped near the end of the runway.
The flight if the pilot would have performed a go-around just after touching down. In this simulated case, it appears that the go-around may have been successful. The accident report concluded that a go-around would probably have been unsuccessful.
The accident board had a total of 15 findings. In summary:
- The investigators found no problems with the aircraft, airport, air traffic control or crew qualifications.
- It was determined that the captain made several wrong decisions involving approach configuration and aircraft go-around and landing capability.
- A successful go-around or landing was possible at different points during the approach and landing.
- With adequate training the captain may have reacted quickly enough to safely stop the aircraft.
The complete text of the accident board findings can be found here: NTSB Findings
A link to the official NTSB report for this accident can be found here: NTSB Report
The NTSB had two recommendations for the FAA related to ensuring that procedures in the operations manuals for airports are current and applicable and to institute a program to emphasize the importance of a continual, critical review and update of airport operations manuals. They also had four separate recommendations to improve accident response at Harry S. Truman Airport.
The complete list of the recommendations is available here: NTSB Recommendations
The 727-100 Series aircraft airworthiness was certified under Civil Air Regulation (CAR) 4b as amended by Special Civil Air Regulation No. SR-422B.
Paragraph 4T-122 landing distance requirements.
14 (CFR) 121.195 "Airplanes: Turbine Engine Powered: Landing limitations: Destination airports" was applicable at the time of the accident. This rule states that the landing distance at the arrival airport must be ≤ 60% of the runway available.

Pilot Culture
Operationally, go-arounds are a rare event. A go-around and subsequent second approach requires extra time and fuel and results in delays. With time-critical airline schedules, flight crews can face significant company pressures to avoid having to perform a go-around. Currently, many airlines have removed the stigma from go-arounds and actively encourage their pilots to do so whenever there is an unstabilized approach or any doubt of a successful landing.
Training
The majority of modern airline flight training is conducted in FAA-qualified flight simulators. As part of this training, all crews are trained on go-around procedures. They are also trained on rejected, or balked landings, in which the airplane momentarily touches down, such as a bounced landing. In training, go-arounds and rejected landings are generally expected, thus losing the "startle" factor which can add to decision time. If a go-around or rejected landing is begun within the touchdown zone (normally the first third of the runway) published missed-approach procedures generally provide adequate terrain clearance. In most cases, when the go-around is initiated after touchdown, the distance to perform a go-around is longer than the distance to perform a maximum-braking, full-stop landing. In this accident, the amount of runway required to conduct a go-around was exacerbated by American Airlines' required procedure to let the engine stabilize at an intermediate thrust setting prior to commanding go-around power. The Safety Board believed and stated in the accident report, that throughout the industry, air carrier pilots may have little knowledge of the distance required to execute a go-around under varying conditions of temperature, elevation, velocity, gross weights, and engine spool-down. Recently, guidance to pilots has emphasized that, once reverse thrust is deployed, there should be no attempt to go around.
American Airlines
At the time of the accident American Airlines was aware of the short runway at St. Thomas, and that landings could, at times, be challenging. The airport was known to often have gusty winds and inaccurate wind reports due to surrounding terrain. American Airlines had released several memos regarding landing at this airport.
The first documentation was a letter to Caribbean flight crews on May 21st, 1971 (note yellow highlights are added to point out relevant portions of the letter). Among the items it emphasized were the wind conditions to be expected, the flap settings to use, the need for accurate and quick touchdown, and the modified procedure to deploy all deceleration devices as soon as possible after touchdown in order to reduce landing distance.
The second was Operations Bulletin FM2 C-7. This was a special bulletin for this airport only. It required the pilot to have three landings with a check pilot before performing operational landings. Investigators determined that this bulletin introduced some confusion regarding landing flap settings. It reads as follows:
- An exception is made to Flight Manual Part One in that DAY VFR approaches are authorized at STT provided the STT weather cloud base is reported at 3,000 feet or more and the visibility is three miles or more and the flight has received approval to make a VFR approach. When approaching STT, from DUTCH or CULEBRA, and having received authorization for a VFR approach -- the course shall be altered to pass over Savannah Island, thence turning left for a straight-in approach to Runway 9. This exception to Part One is not to be construed as endorsing unwise or imprudent operating practices.
- B-727/100 are the only aircraft authorized to serve STT.
- Landings will be made on Runway 9 only.
- All landings and take-offs at Truman Airport will be made by the captain.
- Flap Usage: As a standard practice, 40-degrees flap landings will be made. However, with strong or gusty winds, it is the Captain's option to use 30 or 40 degree flaps for landing.
- With a wind component of 20 knots or more, landing with 30-degree flaps is recommended.
- Tailwind Components for Landing: A tailwind component of four knots wet and six knots dry is authorized and requires the use of 40 degree flaps."
It introduced the underlined word "or" in item (5). Even though the winds reported to the airplane prior to approach were under 20 knots headwind and no report of gusts, which by item (6) should cause the use of Flaps 40, the captain, in post-accident interviews, stated that "he knew that any southeast wind at St. Thomas would be gusty," and therefore he decided to use 30 degrees of flaps.
Airport
The St. Thomas airport was a known short airport, especially for jet transports, which is why American Airlines had special procedures. The local government knew there were safety issues for high performance jets landing on the short runway and there were numerous articles in the local papers proposing to upgrade the airport to make it safer. Conceding that 4,658 feet is shorter than runways at most airports, Donald J. Lloyd-Jones, American's senior vice president for operations said, "Runway length is not the only criterion of safe operation. We would not have been operating in there if we didn't think it was safe." Because the runway is relatively short, "the safety tolerance is less than in other airports. However, it is a safe landing distance. We have had some 4,000 operations there with this kind of equipment."
Also, several other significant runway departure accidents had happened here. Traffic levels were increasing, so, to preclude any further accidents, the Port Authority was recommending a major expansion of the airport to include a new terminal and lengthening the runway to 7,000 feet to more safely accommodate larger jet traffic. In fact, just 11 days prior to the accident the recently appointed new FAA Administrator, Dr. John McLucas, traveled to St. Thomas to be briefed on this proposal, which included a request for Federal funds. Several articles were published in the local newspaper on this event (April 14th, April 15th).
Related Articles: (The Daily News of the Virgin Islands April 14, 1976, The Daily News of the Virgin Islands April 15, 1976)
The captain's failure to follow company procedures:
- The captain did not land the airplane using Flaps 40. This was in part due to his "assumption" regarding the winds he expected to encounter, not the actual reported winds.
- The captain failed to land the aircraft in the desired touchdown area even though it was stressed in company documentation that at this airport it was critical to do so.
- The captain failed to perform a go-around when he did not land in the required touchdown zone.
The Captain was not fully aware of the aircraft go-around and landing performance:
- Once the aircraft was on the ground, the captain lost awareness that he had adequate runway to execute a full-performance stop.
- The captain was not aware of the aircraft go-around performance and initiated a go-around when there was insufficient runway to do so.
- Special company procedures would be unambiguous and adhered to by the
flight crew. These included:- The pilot would use proper flap setting
- The pilot would land in the directed touchdown zone and go around if
landing would be outside the touchdown zone
- The distance to do a go-around is less than the distance to perform a full stop.
Several previous accidents at the St. Thomas airport were cited in the accident report as precursors to the subject accident, pointing to peculiarities of the airport:
Trans Caribbean Airways Flight 505, St. Thomas, Virgin Islands, December 28, 1970
This accident also involved a Boeing 727 on December 28, 1970. The aircraft bounced several times during the landing, struck a wingtip, and ran off the side of the runway. The investigators determined the probable cause to be: "The captain's use of improper techniques in recovering from a high bounce generated by a poorly executed approach and touchdown. Lack of cockpit crew coordination during the approach and attempted recovery contributed to the accident."
View accident report.
Caribbean Atlantic Airlines Flight 340, St. Thomas, Virgin Islands, August 12, 1969
This accident on August 12, 1969, involved a Douglas DC-9-31. This was also a Runway 09 over-run accident with a probable cause of: "... loss of effective braking action caused by dynamic hydroplaning of the landing gear wheels on a wet flooded runway. Contributing factors were a higher-than-normal touchdown speed and the location of the airport and its topography which permitted excess levels of water to accumulate on the runway."
View accident report.
Industry
There was no regulatory action taken by the FAA as a result of this specific accident. However, even though the quality of the approach was not a factor in this accident, it did happen in the landing phase and thus was one of the precursor events that eventually resulted in the industry's Approach and Landing Accident Reduction (ALAR) programs. Results of these initiatives included issuance of the FAA's Flight Standards Bulletin for Air Transportation 01-02 (FSAT 01-12), later superseded by FAA Information for Operators (InFO 08029), Approach and Landing Accident Reduction (ALAR): Recommended Flight crew Training. The InFO's Supportive Information contains an appendix containing the Air Transport Association's ALAR Training Guide. It also points to:
- The FAA's Advisory Circular 120-71A, Standard Operating Procedures for Flight Deck Crewmembers
- The Flight Safety Foundation's ALAR Toolkit (Introduction to Briefing Guide)
The human factors aspects of this accident, in combination with a number of other accidents and incidents, led to the eventual publication of FAA Advisory Circular 120-51, Cockpit Resource Management Training. This AC provides guidelines for 14 CFR parts 121 and 135 certificate holders to establish training designed to increase the efficiency with which flight crew members interact in the cockpit by focusing on communication skills, teamwork, task allocation, and decision making. This AC was later revised on February 10, 1993, as AC 120-51A which changed the name to "Crew Resource Management." This AC has been revised several more times and is currently at revision E (AC 120-51E).
There have also been some cultural changes in the industry. Training includes much more emphasis on having a "mind set" that a go-around could be necessary, thus being more prepared in case the necessity actually arises. Most airlines have also implemented procedures that say once the aircraft has landed and any deceleration devices (speed brakes, thrust reversers...) have been deployed, do not attempt a go-round.
Advances in Airplane Landing Performance
Since the accident, a number of improvements in airplane systems and stopping performance have evolved, and most have become standard equipment on modern transport airplanes. As a demonstration of the improved capabilities resulting from these advances, a visual representation of the accident scenario was conducted in a 737 full-flight simulator. The representation attempts to duplicate the available field length during the accident and illustrates the enhanced landing and stopping capabilities compared to the jet transports flown at the time of the accident. None of the advances demonstrated in this simulation were made mandatory by this or other similar accidents, but were developed as a natural result of technological evolution and advancements in the state-of-the-art of airplane and systems design.

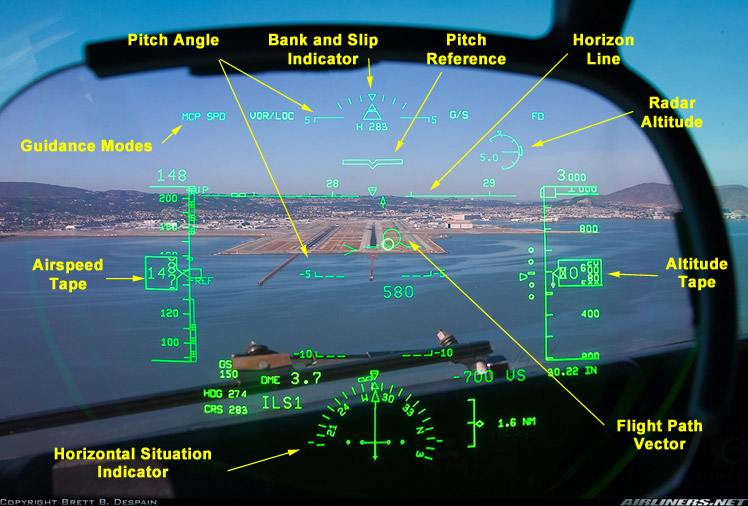
Photo copyright Brett Despain - used with permission
View Larger
{kind=link}
The video depicts a maximum performance full stop after a normal flare and landing using all the modern available safety features listed below, most of these features were not available on the 727 at the time of this accident:
- Automatic Speed Brakes. With this system the speed brakes are automatically deployed when the aircraft lands. Should the pilot move the throttles forward in an attempted go-around, the speed brakes would then stow automatically. Should the automatic system fail, a "SPEEDBRAKE" warning is initiated, prompting the crew to deploy the speedbrakes manually.
- Autobrakes. In this system the brakes can be set to function automatically at touchdown and through a range of deceleration levels.
- Carbon Brakes. Most modern airliners now employ brakes formulated from carbon. Overall, carbon brakes provide better braking performance than the traditional steel brakes used during the accident time frame.
- Thrust Reversers. Although the accident aircraft did have thrust reversers, at that time the engines were much slower to accelerate. In the accident, they were only partially deployed when the airplane overran the runway.
- Autothrottle. All modern airliners now have an autothrottle system. This includes automatic retarding of the thrust to idle when starting the landing flare.
- Head-up-Display (HUD). The use of the HUD allows the pilot to be looking outside at the runway and still have all the basic flight instruments in view, avoiding having to look back inside at flight deck instruments. The photo to the right is a view through a typical HUD. This includes, among other things, a flight path vector (round aircraft-like symbol in the middle), which indicates the aircraft flight path. Flying the airplane to place the flight path vector at the end of the runway will result in touchdown at that point.
American Airlines
As a result of this accident, American Airlines ended all jet flight to St. Thomas, flying instead into St. Croix, where the runway is much longer (7,600 feet). American resumed jet flights into St. Thomas in 1991 after the runway was lengthened to 7,000 feet.
Shortly after this accident, American Airlines published several letters to crews and management to address topics of concern:
The first letter on May 6, 1976 was addressed to the training department and directed them to emphasize stabilized approaches, early touchdown, and go-around performance and techniques/procedures. Applicable statements are highlighted. Of note was the instruction that it takes more runway to do a go-around from idle thrust than it takes to perform a full-stop landing. The letter also emphasized that landing should occur "on or near the 1,000' point". It also discussed demonstrating the length of the go-around in the simulator.
The second letter (Appendix I) (Bulletin 223-76) on May 10, 1976 was addressed to pilots and flight engineers and discussed concerns arising from the accident. Applicable statements are again highlighted. It also emphasized the need for a stabilized approach to accomplish a "spot" landing and to initiate a go-around no later than the target touchdown area (1,000'-1,500' from the approach-end of the runway). It also discussed engine acceleration time for jets to achieve go-around power from idle.
Finally, the airline issued Operations Bulletin FM2 C-13, (replacing C-7 and C-12) which provided more detailed information about St. Thomas operations. It clarified flap usage and included advice on when to initiate a go-around. Specifically, it said, "Go-around shall not be attempted after the aircraft has touched down on the runway, and the landing should be continued to a stop -- recognizing the full stopping capabilities of the 727 with spoilers, main and nose gear brakes."

Airport
Shortly after the accident, the Port Authority received a large Federal grant of $76 million dollars for airport upgrades. Soon thereafter, a long-term airport upgrade was begun, which included:
- A new 7,000-foot runway, just south of the existing runway and accompanying taxiways. This involved extending the runway farther into the bay.
- A new terminal and parking ramp.
The picture to the right is an aerial photo taken during the reconstruction. The Google map below shows the current runway with an overlay outline showing the position of the original runway.

View Larger
Airplane Life Cycle:
- Operational
Accident Threat Categories:
- Crew Resource Management
- Landing / Takeoff Excursions
- Incorrect Piloting Technique
Groupings:
- Approach and Landing
Accident Common Themes:
- Human Error
Human Error
The investigators determined that the captain made several consecutive, significant errors:
- He violated company policy regarding the selection of the landing flap configuration. This decision was a result of his "assumption" regarding the wind conditions and the ambiguous wording of the latest Operations Bulletin.
- The captain's failure to land the aircraft in the required touchdown zone, and his indecision to initiate a go-around once beyond that zone. Once the airplane floated beyond the touchdown zone (as stressed in company policy) he should have immediately initiated a go-around. If a go-around had been initiated at this point, there was sufficient runway to successfully complete the maneuver.
- The captain decided to initiate a go-around in a situation where airplane go-around performance was inadequate. He further was not aware that had a full stop been initiated from the same point on the runway, adequate braking performance was available to successfully stop the airplane on the runway.
- Finally, after initiating the final stop, the captain did not maintain full braking, did not deploy speed brakes, and did not fully deploy thrust reversers, lengthening the resultant overrun.
The following is not an exhaustive list but includes a number of accidents similar in causes to American Airlines 625.
Alaska Airlines Flight 60 at Ketchikan, Alaska
This Boeing 727 accident occurred just 22 days prior to the subject accident. It is related in that it was the same type aircraft and had similar outcome and similar probable cause of pilot incorrect decision-making regarding landing versus a go-around.
View accident report.
United Airlines Flight 227 at Salt Lake City, Utah
This Boeing 727 accident in November 1965 was similar in that it involved a crash on landing that was due in part to the pilot failing to properly manage his landing flare.
View accident module.
World Airways Flight 30H at Boston, Massachusetts
This McDonnell Douglas DC-10 accident in January 1982 was similar in that the crew landed the aircraft long. Realizing they would not stop on the runway, the crew steered off the side of the runway instead of departing at the end.
View accident report.
Federal Express at Newark, New Jersey
This McDonnell Douglas MD-11 accident in July 1997 was similar in that the crash was on landing. The accident was in part due to the pilot’s failure to execute a timely go-around during a destabilized flare resulting from the captain’s concern with touching down early to ensure adequate stopping distance.
View accident report.
American Airlines Flight 1420 at Little Rock, Arkansas
This McDonnell Douglas MD-82 accident in June 1999 was similar in that it was a runway overrun due in part to poor crew decision-making and actions during the attempted landing.
View accident module.
Southwest Airlines Flight 1455 at Burbank, California
This Boeing 737 accident in March 2000 was similar in that it was a runway overrun due to poor crew decision-making and actions during the landing. They approached the runway with too high an airspeed and forced the aircraft to land instead of performing a go-around.
View accident report.
Luxair Flight LG9642 at Luxembourg
This Fokker F27 accident in November 2002 was similar in that it involved poor decision-making and crew actions during an aborted go-around and subsequent landing attempt.
View accident module.
Southwest Airlines Flight 1248 at Chicago Midway
This Boeing 737 accident in December 2005 was similar in that it involved an overrun that was due in part to the crew making poor decisions after touchdown. The crew landed on a contaminated runway and did not deploy all deceleration devices in a timely manner, nor did they attempt a go-around when braking action was almost non-existent.
View accident module.
Pinnacle Airlines Flight 4712 at Traverse City, Michigan
This Canadair Regional Jet CL600 accident in April 2007 was similar in that it was a runway overrun at least partly caused by numerous pilot errors during the approach and landing.
View accident report.
Delta Connection Flight 6448 at Cleveland, Ohio
This Embraer ERJ-170 accident in February 2008 was similar in that the aircraft landed long when the crew lost track of their position on the runway and failed to execute a missed approach.
View accident report.
East Coast Jets Flight 81 at Owatonna, Minnesota
This Hawker Beechcraft 125 accident in July 2008 was similar in that it involved an overrun accident when the crew attempted a go-around with insufficient runway remaining.
View accident report.
Air France Flight 358 at Toronto Canada
This Airbus A340 accident in August 2005 was similar in that it involved a runway overrun caused in part by the crew's failure to abort the landing and perform a go-around after finding themselves outside normal parameters over the threshold.
View accident report.
Technical Related Lessons
Flight crew awareness of landing and go-around performance and the critical differences in associated field length requirements is essential to safe operations. (Threat Category: Incorrect Piloting Technique)
- The decision on whether to perform a landing or go-around is dependent on the pilot's knowledge of the aircraft's performance capability. In this accident, the pilot was not aware that once the aircraft was on the ground the remaining runway was sufficient to complete a full stop. He was also unaware that the distance to perform a go-around is longer than a stop, and that he most likely did not have sufficient runway to conduct a go-around. Investigators determined that this lack of knowledge contributed to his incorrect decision making. Investigators further concluded that with adequate training related to the airplane's performance capability after touchdown, the captain may have reacted immediately to stop the aircraft instead of attempting a go-around.
During landing operations, especially in situations where available field length is a limiting consideration, flight crews need to maintain an awareness of their relative position on the runway. If landing will occur beyond the designated touchdown zone, a go-around should be initiated, and once on the ground, a full stop using, if necessary, the maximum performance capabilities of the airplane, should be conducted. (Threat Category: Landing/Takeoff Excursions)
- It is imperative to land within the required touchdown zone to avoid the possibility of an overrun, especially on short runways where performance may be limited. Typical airline guidelines are to touch down in the first third of the runway. At the time of this accident, American Airlines had a more stringent requirement to land within 500 feet of the 1,000-ft. aim point. The captain violated this requirement by floating for seven seconds prior to touchdown and landing more than 1,000' beyond the required touchdown zone.
Crew Resource Management should be integral to flight crew training. (Threat Category: Crew Resource Management)
- Human factors studies have shown that when complex, time-critical safety decisions must be made, humans will channel their attention and situational awareness will degrade, leading to an increase in errors. For this reason, having multiple crewmembers complementing each other is a widely accepted safety aid. In this accident, all three flight deck crewmembers knew of the short runway and the associated company procedures, but none of the non-flying crewmembers spoke up or prompted the pilot to initiate a go-around when the airplane flew past the required touchdown zone.
Common Theme Related Lessons
Adherence to standard operating procedures and specific company procedures, especially when operating on performance-limited runways, is essential to maintaining safe operations. (Common Theme: Human Error)
- Landing and stopping performance is highly dependent on the airplane landing configuration, touchdown point, and actuation of deceleration devices. In this accident the pilot failed to follow company guidelines by: landing with the incorrect flap setting; landing beyond the designated touchdown zone; and failing to perform a go-around once having transited the touchdown zone without landing. Once the pilot did commit to stop, all available deceleration devices were not deployed, and full braking was not maintained while on the airport paved surface.