
Boeing Model 727-22

United Airlines Flight 227, N7030U
Salt Lake City, Utah
November 11, 1965
United Airlines Flight 227, a Boeing 727, crashed during an attempted landing at Salt Lake City Airport. The captain failed to recognize and arrest an excessive sink rate on final approach, resulting in a touchdown 335 feet short of the runway. The main landing gear sheared off, causing a breach in the fuselage, and the airplane caught fire while sliding down and off the right side of the runway. Failure of the main landing gear ruptured fuel lines and generator leads, causing the fire. The entire roof and cabin area forward of the fuselage breach was consumed by fire. Of the 85 passengers aboard, there were 43 fatalities. All six crew members survived. The Civil Aeronautics Board (CAB) determined that the accident was survivable - none of the passengers sustained any traumatic injuries that would have precluded their escape. The 43 fatalities were attributed to the fire caused by the broken fuel line. The CAB also established that similar future events could not be ruled out, and that the airplane should be designed to have a higher degree of survivability in these types of events.
On November 11, 1965, United Airlines Flight 227, a Boeing 727, crashed during an attempted landing at Salt Lake City Airport. The captain failed to take timely action to arrest an excessive descent rate during final approach. After touching down 335 feet short of the runway, the main landing gear sheared off and the airplane caught fire. The airplane then slid 2,800 feet on the nose gear and bottom of the fuselage, stopping 150 feet off the right side of the runway.

Photo Copyright Bruce Leibowitz - used with permission
Severe upward and rearward impact forces from the right main landing gear assembly produced a large impact hole in the fuselage and ruptured fuel lines and the number 3 generator leads on the right side of the fuselage. The fuel was ignited by sparks from the fuselage scraping on the runway, and/or the severed generator leads. The hole and fire damage area extended circumferentially from the lower sill of the aft cargo compartment door to the airplane nose. The entire roof and cabin area forward of the fuselage breach were consumed by fire, which was initially being supplied fuel under pressure by the operating boost pumps. All flight control cables, fuel supply lines from the number 2 and 3 tanks, and the number 3 generator leads, which were routed through the cabin floor beams in the area of the impact hole, were consumed by fire. Only a 5/8-inch stainless steel hydraulic pressure line remained intact. Of the 85 passengers aboard, there were 43 fatalities. All six crew members survived.
History of Flight
On the day of the accident, Flight 227 departed New York's LaGuardia Airport for its eventual destination of San Francisco, California. Enroute stops were planned in Cleveland, Ohio, Chicago (Midway Airport), Illinois, Denver, Colorado, and Salt Lake City, Utah. A crew change was accomplished in Denver.
The flight to Salt Lake was uneventful prior to the approach for landing. Upon being cleared for the Instrument Landing System (ILS) approach, while at 10,000 feet altitude and 250 knots indicated airspeed, the flight notified the air traffic controller that they had the runway in sight, and subsequently cancelled their instrument flight rules (IFR) clearance but remained on the controller's radio frequency for traffic advisories. Within a minute, the flight control had been transferred to Salt Lake Tower, and a clearance to land was issued. Three minutes later, the airplane crashed. The accident occurred in darkness at 5:42 PM local time.
Earlier in the approach, while in a descent at 16,000 feet, the pilot flying reduced all engines to idle thrust and extended the speed brakes in order to expedite descent. At 11,000 feet, the speed brakes were retracted at approximately the same time the field was sighted. Speed reduction was continued, with the landing gear and flaps being extended until achieving the final landing configuration of 40 degrees of flaps, landing gear extended, and a speed of 123 knots. In the final landing configuration, the descent rate of approximately 2,300 feet per minute was maintained, and a full "fly-down" command was indicated by the flight director (flight instruments), indicating that the airplane was high on the glide slope. A normal descent rate for landing would be approximately 800 feet per minute, while established on the glide slope, at the intended approach speed.
According to the CAB report, between 90-120 seconds prior to impact, the first officer, who was flying the airplane, attempted to increase thrust, but was prevented by the captain, who commented, "not yet...." Approximately 30 seconds later, the first officer advanced the throttles to approximately half their travel but did not sense an engine response. At this point he again reached for the throttle, intending to advance them to full travel, but the captain had already done so and had taken control of the airplane. The throttles were advanced to their maximum approximately five to ten seconds, but not more than 15 seconds prior to impact. Flight crew members reported hearing the engines respond in a manner consistent with an increasing thrust. Many survivors and cabin crew members also reported hearing the engines "spool up" prior to impact. Early-era jet engines tended to have slow acceleration times and were only required to reach takeoff power within eight seconds of throttle movement, after having been stabilized at idle. The acceleration characteristics determine how the airplane satisfies go-around climb requirements and may determine the maximum allowable landing weight of an airplane, based on the combination of available thrust and airplane gross weight. In this accident, given the acceleration characteristics of the engines, if the initial throttle movement occurred in as little as five seconds prior to impact, the engines would not have had time to accelerate to a thrust level sufficient to arrest the sink rate. Even if the command to accelerate had occurred 15 seconds prior to impact, this was still not sufficient to arrest the sink rate and avoid the hard impact with the ground.
The investigation determined that all three engines had been capable of producing rated thrust prior to impact, and only two of the eight fuel boost pumps, each from a different tank, failed to meet specifications. Engine bleed valves were all tested and found satisfactory. All three engine fuel controls were found to be functioning normally, although the control for the number 3 engine produced an engine response that was one second slower than the other two engines. The fuel tanks remained intact, and all fuel shutoff valves were open. All three engines sustained heavy foreign object damage. An animation of the accident sequence is available below:
Flight Crew Training
The CAB placed the responsibility for the accident entirely on the captain and his failure to adequately monitor and arrest the excessive descent rate prior to impact.
The CAB discussed at length his inconsistent training record in jet aircraft, noting that in February of 1961, his jet training was terminated based on "unsatisfactory performance in the areas of command, judgment, standard operating procedures, landing technique, and smoothness and coordination." Subsequent evaluations upon returning to jet training in May 1962 continued to show inconsistencies, and though becoming type rated in the 727, some of those inconsistencies, such as being high on the glide slope during instrument approaches and being slow to add power during go-around situations, were similar to circumstances leading to the accident.
Following the accident, the FAA issued an order requiring all Principal Operations Inspectors to review their assigned carrier's operating procedures and approved training programs. This included requirements that all operations manuals include procedures to increase pilot awareness of altitude and descent rates. The order also imposed training requirements for a high rate of descent demonstration by pilots in command of turbojet aircraft, to demonstrate the undesirable landing approach profile and its effects. Additionally, flight time requirements were established for the captain before the captain could allow the copilot to execute a takeoff, approach, or landing. Also, the minimum numbers and types of landings were increased for pilots receiving their initial checkout in turbojet equipment. Additional emphasis was placed on training in the proper use of artificial horizons and flight directors and the attitudes necessary to maintain level flight in various flight conditions.
Passenger Evacuation
The CAB determined that this accident was survivable. Of the 91 persons on board, 50 successfully evacuated the airplane, although many were severely burned and others sustained injuries during egress. The 41 passengers who did not escape were overcome by dense smoke, heat, and flames.
All of the emergency exits were available and were used. As the airplane skidded to a stop off the side of the runway, many passengers moved forward to the main cabin door. The press of passengers crowded in the door area prevented the flight attendant from immediately opening the door. The second officer (flight engineer) exited the flight deck and was able to open the door, inflating the slide. He began directing the evacuation of passengers. The captain and first officer escaped via the operable flight deck side windows, and they did not shut down the engines prior to exiting. During the investigation, it was determined by the CAB that the flight deck remained configured consistent with flight. The captain and first officer did not actuate any switches or controls prior to leaving the airplane.
On the right hand side of the airplane, the galley door, between seat rows eight and nine and the over-wing emergency exits between rows 12 and 14 on both sides of the airplane were all opened by passengers. The galley door escape slide could not be deployed by the passenger who opened the door, and a flight attendant who had been riding as a passenger instructed him how to deploy the slide. Both were outside the airplane at the time.

and two passengers were rescued. (Aft airstair is at left)
When the airplane came to a complete stop, the flight attendant occupying the aft passenger door jumpseat opened the door to see if the aft airstair was available for egress. The nose-high attitude of the airplane, resulting from the loss of the main landing gear and extended nose gear, prevented the airstair from opening more than about six inches. Two men who were seated in the aft cabin area had preceded her into the stairwell, and when all three of them attempted to return to another exit, their passage was blocked by fire and smoke. All three moved as far into the stairwell as possible and began pounding on the side of the fuselage and yelling to fire crews outside the hull. The flight attendant extended her arm through the small airstair opening and was able to attract the attention of fire crews who passed a fire hose through the opening. One of the passengers who was trapped with the flight attendant used this fire hose to spray the surrounding area. Eventually, all three were rescued through the large hole that had burned through the aft cabin wall on the right hand side of the airplane. Both passengers subsequently died in the hospital, seven and eleven days following the accident.
The CAB issued nine findings and determined that the probable cause of the accident was, "...the failure of the captain to take timely action to arrest an excessive descent rate during the landing approach."
The specific findings issued by the CAB were (quoted directly from the accident report):
- The aircraft, powerplants, and all systems were capable of normal operation.
- The aircraft crossed the outer marker over 2000 feet above the ILS glide slope.
- The rate of descent during the final approach exceeded 2000 feet per minute, approximately three times the United Air Lines recommended rate of descent for landing approaches.
- The captain stopped the first officer's initial attempt to apply power.
- The power applied was applied too late to arrest the rate of descent and make a normal landing.
- The captain's training records indicate a tendency to deviate from acceptable standards and tolerances.
- The right main landing gear severed fuel lines and a cabin fire erupted seconds after impact.
- All emergency exits were used.
- This was a survivable accident.
View the CAB report on this accident.
The CAB issued the following recommendations in the final report:
- The board is concerned that the procedures for pilot testing prevailing at the time of this accident were such that an individual with the pilot behavioral characteristics of the pilot in this case could qualify and be retained as pilot-in-command of a Boeing 727 aircraft. The board therefore recommends that both the FAA and the air carriers reexamine existing procedures to the end that all feasible steps may be taken to make sure that airmen who serve as pilots-in-command of commercial aircraft, and in particular high-speed jet aircraft such as the Boeing 727, possess not only the requisite technical skills, but the necessary qualities of prudence, judgment, and care as well.
- The board believes that all operators of the Boeing 727 should review the decision of United Air Lines relative to positioning of flight attendants near exits, with a view toward adopting that practice.
- The board is also concerned about the loss of life in this survivable accident and recommends that the crash fire prevention research programs underway be pressed with vigor, and that each improvement be incorporated at the earliest possible moment.
Additionally, in a letter to the FAA issued November 30, 1965, and included as an attachment to the official report, the CAB made the following recommendations concerning the Boeing 727:
- Fuel lines through the fuselage should be rerouted so that they pass through the floor beams near the centerline of the aircraft.
- The fuel lines and their shrouds should be made of stainless steel and should have a wall thickness of sufficient dimension to withstand rather severe impacts. The wall thickness should be not less than 0.040 inch.
- The generator leads should be routed so that there is maximum separation between these leads and the fuel lines. Each lead should be in a separate plastic conduit with suitable strength and flexibility to withstand bending and reasonably high tensile load.
Finally, the CAB also recommended that all other similarly configured aircraft (e.g., DC-9, Lear Jet, Caravelle, BAC 111, Jet Commander) be the subjects of a study to determine whether or not analogous dangers existed in their fuel and electrical system geometries.
The Boeing Model 727-200 was certified using Part 4b of the Civil Air Regulations (CAR 4b). While the accident resulted in changes to 14 CFR 25, as it was the effective regulation at the time of the accident, the certification basis for the 727 was accomplished under the regulations in effect at the time of application for type certificate. The following regulations were pertinent to this accident:
CAR 4b.330, .331, and .332, which specified the requirements for the landing gear.
CAR 4b.362, which addressed emergency evacuation.
CAR 4b.381, which specified certain flammability requirements for cabin materials.
CAR 4b.385, which addressed ignition of flammable fluids or vapors.
CAR 4b.432, which addressed fuel lines and requirements for flexibility. This regulation was particularly important in its relation to this accident. The regulation requires that for sections of fuel lines where relative motion may exist, that flexibility between the sections (i.e. flexible connections) and/or flexible hose was required to prevent fuel leakage. Relative to this accident, the ruptured fuel lines were in areas where the flexibility was not required. As a result, the fuel lines ruptured, releasing fuel under pressure (the fuel boost pumps continued operating for a period during the initiation of the fire), which was ignited by either sparking generator leads, sparks from the fuselage on the runway, or both.
CAR 4b.626, which addressed electrical fire and smoke protection.
In 1965, after the certification of the 727, CAR 4b was replaced by 14 CFR part 25 (FAR 25) as the certification standard for transport airplanes. The 14 CFR 25 counterparts of CAR 4b Boeing 727 certification basis were modified following this accident. Reference the section addressing "Resulting Regulatory and Policy Changes" to view the affected regulations.
Airplane Characteristics
The Boeing Model 727 was a relatively new airplane in service at the time of this accident, having been in airline service since February of 1964. As a result, crews were still being trained and transitioning into the 727. The 727 was designed with an operational capability that allowed it to be operated into and out of shorter runways than its predecessor airplanes such as the 707 and DC-8. The short field capability was the result of a sophisticated high lift system that allowed slower takeoff and landing speeds, but that also could result in very high descent rates due to the high drag levels associated with the high lift system. Further, the high descent rates could develop rapidly, requiring crew awareness and monitoring to control and arrest sink rates before inappropriately high levels could develop. This was a characteristic of the airplane that was well understood throughout the industry, but that could surprise flight crews that were new to the airplane. Both the captain and first officer on the accident flight were relatively new to the airplane, the captain having 334 hours in the 727 and the first officer only 84. The CAB stated in its final report that the captain had allowed the sink rate during final approach to become excessive, and he did not take timely action to arrest the sink rate and thereby prevent the crash. Also, at the time of the accident, Ground Proximity Warning Systems (GPWS) had not been developed and were not standard equipment on any commercial aircraft of the era.
Crew Resource Management
In 1965 when this accident occurred, Crew Resource Management (CRM) was not an industry standard for aircrew interaction. No formal training programs existed for CRM, and no airline policies included CRM as a standard practice. The result was an autocratic system where the captain was the primary, and sometimes only, decision maker in the flight deck. The authority of the captain was rarely, if ever, questioned. In this accident, the first officer was flying the airplane and became uncomfortable with the way the approach was progressing. He attempted to increase thrust, to either arrest the sink rate or to initiate a go-around. The captain overrode the first officer and prevented him from advancing the throttles. This allowed the sink rate to further increase, and when the captain finally intervened and advanced the throttles himself, it was too late to arrest the sink rate and avoid ground impact short of the runway.
Cabin Crew Seating
Prior to this accident, it was a standard practice to seat cabin crew members (flight attendants) anywhere in the cabin where seating was available. As a result, following the crash, in which all passengers survived, the rush to the emergency exits prevented flight attendants from immediately reaching the exits themselves. This prevented a timely opening of emergency exits and allowed the fire to spread before the evacuation began. The CAB cited the cabin crew seating arrangements as a factor in the loss of lives due to the post-impact fire. Following the accident, one of the flight attendants who had survived the accident recommended that flight attendants be seated near the exits for all takeoffs and landings. This was adopted as a standard practice by United Airlines and is now a standard practice throughout the industry.
The following key safety issues contributed to this incident:
- Rigid metal fuel lines within the fuselage with no provision for deformation during a survivable accident.
- Inadequate design, procedures, and training to maximize passenger survivability after a survivable accident.
- Inadequate training for piston airplane pilots to transition into jet airplanes, which are less forgiving during approach and landing.
- The seating of the crew's three flight attendants away from emergency exits, which would preclude them from reaching those exits in time to assist in passenger evacuation.
The following design and safety assumption contributed to this accident:
- Occupants would be able to evacuate the airplane safely following a crash landing with less than a catastrophic impact.
Two previous accidents, a United Airlines DC-8 in Denver, Colorado in July 1961 and a Trans World Airlines Boeing-707 in Rome, Italy in November 1964, indicated that the existing regulations relating to occupant survival and passenger evacuation were not adequate. After these two accidents, the FAA was aware of the need to upgrade the regulations in the emergency evacuation and cabin safety areas and was evaluating regulatory changes when the flight 227 accident occurred. This accident prompted quicker action and led to Amendment 25-15 which changed many cabin safety regulations.
As a result of the United Flight 227 accident, the following regulatory changes were made:
- A new section of 14 CFR 25.993(f) was added by Amendment 25-15. That section states, in part; "Each fuel line within the fuselage must be designed and installed to allow a reasonable degree of deformation and stretching without leakage." This regulatory change was the result of a CAB recommendation that fuel lines be constructed of stainless steel and be of at least a certain thickness. The intent of the recommendation was to preclude fuel line rupture and fuel leakage in a situation similar to the circumstances of flight 227 and was based on the fact that a single 5/8-inch diameter stainless steel fuel line remained intact after the accident. In reviewing this recommendation, the FAA determined that fuel line flexibility would provide a more positive means to preclude fuel line ruptures and leaks, and therefore adopted this requirement rather than the specific CAB recommendation.
The regulatory preamble material discussing the rule amendment stated specifically that the intent of the rule was to prevent fuel leakage and fire following separation of the landing gear. In order to demonstrate compliance with this new requirement, one manufacturer developed a test procedure and test apparatus to verify the rupture resistance of fuselage fuel lines.
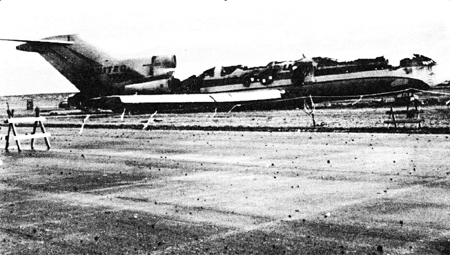
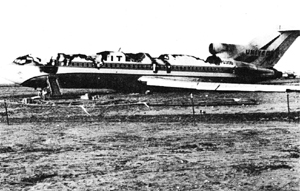
Following implementation of this new rule and incorporation of an Airworthiness Directive mandating flexible fuel lines, a number of incidents proved the effectiveness of the modification. These two photographs show catastrophic fuselage damage but no evidence of fire, which would have resulted if the fuel lines had been broken.


Photo of catastrophic fuselage damage
- Notice of Proposed Rule Making (NPRM) proposed to include shrouding of the fuel lines. It was not included in final rule because shrouding was already required by section 14 CFR 25.863.
- Special Retroactive Requirements, 14 CFR 25.2(a) was added to require compliance to, among other things, 14 CFR 25.993(f) retroactively, along with many cabin safety, fire protection, and occupant evacuation regulations. Also, 14 CFR 121 was extensively revised to incorporate many of the 14 CFR 25 requirements into the existing fleet.
- In January 1966, the FAA established an Agency Task Force to review the factors affecting crashworthiness and passenger evacuation in light of this accident and make recommendations on regulatory changes needed. The Agency also held a public conference in April 1966 to review the airworthiness standards for part 25 airplanes. In addition to the 14 CFR 25 regulation changes by Amendment 25-15, many 14 CFR 121 regulations were changed to require that many of the 14 CFR 25 crashworthiness and passenger safety design features be retroactively included in the existing commercial transport airplane fleet.
- Amendment 25-15 included changes to: 14 CFR 25.721 which covers design of main landing gear such that its failure due to overloads is not likely to puncture any part of the fuel system in the fuselage. 14 CFR 25.803 included the requirement for a 90-second evacuation demonstration in Part 25 and revised the Part 121 requirement from 120 seconds to 90 seconds. 14 CFR 25.807 revised the exit size requirements. 14 CFR 25.809 added design criteria for evacuation slides. 14 CFR 25.812 included requirements for interior and exterior emergency lighting for night passenger emergency evacuation. 14 CFR 25.813 covered design feature in emergency egress paths. 14 CFR 25.853, 25.1359, and Appendix F added additional flammability test criteria and testing methods of interior materials and wiring. Amendment 121-30 to 14 CFR 121 was issued in conjunction with Amendment 25-15 to 14 CFR 25 and added many of these same part 25 changes to part 121.
- Amendment 25-32 made additional changes to 25.721.
- Though not mentioned in the CAB report, shortly after this accident, the industry began development and implementation of Ground Proximity Warning Systems (GPWS), that would, in part, provide a warning if descent rate is too high when close to the ground, and allow sufficient time for recovery. This accident was one of many that led to the adoption of 14 CFR 121.360 that in 1975 mandated the incorporation of GPWS into U. S. commercial aircraft.
As a result of this event, AD 66-30-02 was issued. It required replacement of aluminum fuel lines in the fuselage with flexible fuel lines, and rerouted generator leads.
Airplane Life Cycle:
- Operational
Accident Threat Categories:
- Crew Resource
- Management
- Incorrect Piloting Technique
- Uncontrolled Fire / Smoke
- Cabin Safety / Hazardous
- Cargo
- Landing / Takeoff Excursions
- Excursions
Groupings:
- Approach and Landing
- Loss of Control
Accident Common Themes:
- Organizational Lapses
- Human Error
- Flawed Assumptions
Organizational Lapses
At the time of this accident, it was not common for flight attendants to be seated near emergency exits for takeoff and landing. As a result, in this accident, as passengers gathered near the emergency exits, the flight attendants were hampered in reaching the doors, and door opening, and subsequent evacuation were delayed. Following this accident, it became standard practice to station flight attendants at exits for takeoff and landing so that, in a survivable accident, opening of emergency exits would be immediate.
Human Error
As previously stated, the CAB cited the pilot's actions as the primary cause of the accident. The captain allowed an excessive sink rate to develop, and he did not properly monitor or take timely action to arrest the sink rate and thereby preclude the accident.
Also, when the aircraft came to a stop, the captain and first officer left the airplane via the flight deck side windows. They did not shut down the engines or accomplish any pre-evacuation checklist items prior to departing. The CAB stated in the accident report that the flight crew ".... did not actuate any switches or controls prior to leaving the aircraft."
Flawed Assumptions
It was assumed that, following an accident with less than catastrophic consequences, passengers would be able to successfully evacuate the airplane. Two factors cited by the CAB prevented a successful evacuation: the seating of the flight attendants away from emergency exits, and subsequently their inability to expedite the opening of those exits, and the construction and routing of fuel lines that ruptured and fed the fire following impact.
As related in the Precursors section of the summary, there were two accidents in which passengers died during the evacuation period as a result of evacuation difficulties.
United Airlines Flight 811, Douglas DC-8, N8040U:

The first accident, a United Airlines DC-8, occurred in July 1961 at Denver, Colorado.
The airplane suffered multiple hydraulic failures enroute from Omaha, Nebraska. On landing at Denver, the airplane departed the right side of the runway upon application of reverse thrust on the inboard engines. All tires were blown on the right main landing gear, and all but one tire on the left main gear were blown. The airplane came to rest between the runway and a taxiway. Engines 1, 2, and 4 were separated from the airplane, and, though its mounting hardware had failed, engine number 3 remained with the airplane. At some point during the runway departure, all landing gear (both mains and nose gear) separated from the airplane. Fire broke out on the left wing, destroying a major portion of the left wing and the left side of the fuselage from the cockpit to the aft passenger loading door. Sixteen passengers died as a result of carbon monoxide poisoning when the aircraft burned, and an elderly passenger died following the accident as a result of injuries suffered during the evacuation. The CAB accident report is available at the following link: (CAB report of UAL 859)
Trans World Airlines Flight 800, Boeing 707-331, N769TW:
The second accident occurred in Rome, Italy, in November 1964, and involved a Boeing 707 operating as Trans World Airlines Flight 800. During takeoff roll the crew noticed a failure indication on the number 4 (right outboard) engine, accompanied by a thrust reverser deploy light on the number 2 (left inboard) engine. The crew elected to discontinue the takeoff. The last 1,800 feet of the runway was closed for maintenance, and as the airplane entered this area during the subsequent stopping attempt, it struck a piece of heavy equipment near the right side of the runway. The right wing caught fire and subsequently exploded, spreading the fire to the center cabin area. This was followed by a second explosion that engulfed the entire airplane in flames and precluded further evacuation. The explosions and fire effects resulted in the almost total destruction of the passenger cabin. Of the 62 passengers on board, 45 died in the accident.
In October 1970, the Civil Aeromedical Institute (CAMI) published a report entitled "Survival in Emergency Escape from Passenger Aircraft." This report details not only the two related accidents, but also contains extensive information relative to flight 227. The report is available at this link (CAMI Report) and discusses the survivability aspects of each of the three accidents.
Technical Related Lessons:
Post crash survivability can be greatly compromised by uncontrolled fuel leaks. (Threat Category: Cabin Safety/Hazardous Cargo)
- The Civil Aeronautics Board determined that this accident was survivable, and that no passengers suffered crash-related injuries that would have prevented their safe evacuation from the airplane. However, broken fuel lines, feeding fuel under pressure, combined with sparks from runway contact, or broken and shorted generator leads, or both, led to a fire. This fire prevented the evacuation of nearly half the passengers. Subsequent rule changes required flexible fuel lines that could withstand the forces associated with this kind of accident and provide an additional safeguard against post-crash fires.
Flight attendants should be stationed at emergency exits for takeoff and landing (Threat Category: Cabin Safety/Hazardous Cargo)
- Not all flight attendants were stationed at emergency exits and were therefore not all able to reach their assigned evacuation stations following the accident. Though all emergency exits were used, some were opened by passengers. The forward left main door was opened by the flight engineer, following difficulties experienced by the flight attendant due to the number of passengers gathered at the door. Had all the flight attendants been properly situated and improved assist space been available to access the overwing exits, the passenger evacuation may have progressed more rapidly, resulting in fewer fatalities. Current regulatory requirements specify that during taxi, takeoff, and landing that flight attendants shall be located "as near as practicable to required floor level exits...."
Proper application of threat resolution is dependent upon accurate assessment of the threat and matching the design solution to the actual threat condition. (Threat Category: Uncontrolled Fire)
- The intent of the regulatory changes following this accident was to provide fuel lines that are sufficiently robust to withstand the forces associated with an accident that is otherwise survivable. However, the Civil Aeronautics Board recommended that fuel lines be strengthened and manufactured from stainless steel, in order to withstand accident forces. The FAA disagreed with that recommendation, and instead required fuel lines that were flexible and tolerant of much more deformation than rigid steel lines would have been. Subsequent to implementation of these rule changes, a number of survivable accidents have occurred where the fuel lines remained intact. The eruption of fires due to fuel leaks was prevented in accidents where the fuselage was substantially damaged or even destroyed. Making the fuel lines from stainless steel, and more rigid seemed, on the surface, a desirable change. However, the incorporation of fuel lines that are more tolerant to deformation has proven to be an effective solution.
Flight crew training for new airplanes, especially those incorporating new/unique technology or operational characteristics, should emphasize the unique characteristics of the new equipment. (Threat Category: Incorrect Piloting Technique)
- The Boeing 727 was specifically designed for access to shorter runways, and with a high lift system that would allow low speed, high angle descent. One aspect of the high lift system was that it also created very high drag levels to facilitate the high descent angles. However, this could also lead to very high descent rates. The Civil Aeronautics Board cited as the primary accident cause, the captain's ".... failure to monitor and arrest the excessive descent rate...." Both pilots were relatively new to the airplane (the first officer with only 84 hours of experience in the airplane), and inexperienced with the descent capabilities of the airplane. The FAA later adopted changes to training requirements aimed at preventing the types of operational mistakes that led to this accident.
Non-stabilized approaches add risk to the final phases of landing (Threat Category: Incorrect Piloting Technique)
- This accident was, in part, the result of a non-stabilized approach involving a high descent rate and very low power setting. Had the crew properly monitored their flight path, the approach could have been discontinued at an earlier point, and the accident possibly avoided.
Common Theme Related Lessons
Proper application of a pre-evacuation checklist reduces risk during passenger/crew evacuation following a survivable accident. (Common Theme: Human Error)
- Following this accident, after the airplane had come to a stop, the captain and first officer escaped the airplane through the flight deck windows, which could be opened. They did not employ any checklists and departed the airplane prior to shutting down the engines. The running engines continued to supply electrical power to the fuel boost pumps, thereby feeding the growing fire. Had the engines been properly shut down, the fuel fed fire would have been less intense.