
McDonnell Douglas DC-8-61

Photo copyright George W. Hamlin - used with permission
United Airlines, Flight 173, N8082U
Portland, Oregon
December 28, 1978
On December 28, 1978, a McDonnell Douglas DC-8-61 turbofan powered airplane operated by United Airlines and registered as N8082U, crashed into a wooded suburban area while on approach to Portland International Airport, Portland, Oregon.
Upon approach to Portland International Airport, the aircraft experienced a landing gear malfunction indication and could not determine if the landing gear had been safely extended. The flight crew elected to hold at 5,000 feet to troubleshoot the landing gear anomaly and prepare the aircraft for an emergency landing. With one exception, about 38 minutes into the hold, little was said concerning the amount of fuel onboard and what was needed to complete the approach to the airport. Approximately one hour after beginning the hold, and during the approach to the airport, the aircraft ran out of fuel and crashed approximately six miles northeast of the airport.
Of the 189 people onboard the aircraft, ten were killed and 23 were seriously injured.
History of Flight

Photo copyright Chris Coduto - used with permission
View Larger
{kind=link}
On December 28, 1978, a McDonnell Douglas DC-8-61 turbofan powered airplane, operated by United Airlines and registered as N8082U, crashed into a wooded suburban area while on approach to Portland International Airport (PDX), Portland, Oregon.
The aircraft ran out of fuel while on approach to PDX after the flight crew had spent considerable time troubleshooting an apparent landing gear malfunction, as well as preparing the aircraft and passengers for an emergency landing.
When the landing gear was initially extended on approach into Portland, the right main landing gear retract cylinder assembly pulled apart due to corrosion on the mating threads between the rod end and the piston rod. This allowed the right gear to free fall while the left gear extended normally.
The resulting abnormal noise, vibration, and transient asymmetric drag immediately indicated a failure to the flight crew. Knowing something abnormal had happened and being unable to verify that the landing gear was down and locked, at 17:12:20, when requested by Portland Approach to contact Portland tower, the captain stated: "Negative, we'll stay with you. We'll stay at five. We'll maintain about a hundred and seventy knots. We got a gear problem. We'll let you know."

Photo copyright Capt. David O. Hill – used with permission
The DC-8 landing gear is extended and retracted by moving a handle in the cockpit. For gear extension, the handle is moved down, and the landing gear uplocks are released, allowing gear extension. When the gear is properly extended and locked down, three green lights near the landing gear handle indicate that the landing gear is safe for landing. If the gear extends improperly, or does not lock down for some reason, a red light for the specific gear will illuminate, indicating that the particular landing gear is not extended and/or locked. For retraction, when the cockpit handle is moved up, the gear retraction system is hydraulically pressurized and the retract piston retracts, pulling the associated landing gear assembly into its wheel well. When the retraction is complete, hydraulic pressurization is turned off. On the accident airplane, when the gear was extended, the retract piston became disconnected (or had been disconnected prior to extension), which resulted in unusual noises and an indication that the gear had not properly extended and locked.
The flight crew elected to delay their landing while they investigated the landing gear problems. At this time there was approximately 13,332 pounds of fuel remaining on board.
Throughout the subsequent delay, Flight 173 remained at 5,000 feet with the landing gear down and flaps set at 15 degrees.
Under these conditions the NTSB estimated that the airplane would have been burning fuel at the rate of about 13,209 pounds per hour (220 lbs./min.).
View the National Transportation Safety Board (NTSB) Accident Report.
The DC-8 flight deck has both engine fuel flow and fuel tank quantity indications available to the flight crew. These instruments would have provided enough information for the crew of Flight 173 to determine that they had approximately one hour of flying time left under those conditions.
For approximately the next 54 minutes, the flight crew's attention was focused primarily on the landing gear problem, as well as in the preparation of the passengers and cabin for the possibility of a landing gear collapse during landing.
While the remaining fuel quantity was occasionally noted by the flight engineer during the subsequent 54 minutes, at no time did any of the crew relate the fuel remaining and fuel use rate to the flying time required to reach the airport. In addition, the crew did not discuss the potential of having to perform a missed approach or a go-around and return to land.
View the fuel time line report.
The only indication given by a crewmember on the fuel state was at 17:50:34, some 38 minutes into the hold, when in response to the captain's request: "Give us a current card on weight, figure about another fifteen minutes," the flight engineer told the captain: "Fifteen minutes is gonna --- really run us low on fuel here."

Photo copyright Jeff Schroeder - used with permission
Over the period between 18:06:40 and 18:13:21 all four engines failed. The number 4 engine was the first to fail. Review of the discussion in the flight deck made it clear to the investigators that at least the captain and flight engineer were surprised by the fuel exhaustion. The captain repeatedly asked "Why?" when informed that they were losing an engine. The flight engineer stated, "Five thousand in there ... but we lost it." The number 3 engine was the next to fail, reportedly followed by the near-simultaneous failures of engines 1 and 2.
At approximately 18:15:00, the aircraft crashed into a wooded section of a populated area of suburban Portland about six nautical miles east southeast of the airport. After striking several trees, an unoccupied house, and high tension power lines, the fuselage of the airplane came to rest between some trees and on top of another unoccupied house. There was no post crash fire. The wreckage path was about 1,554 feet long and about 130 feet wide.
The fuselage, from about the fifth row of passenger seats forward, sustained severe impact damage. The cockpit upper structure, which included the cockpit forward windows, had separated and was found to the right of the fuselage just forward of the inboard end of the right wing. The cockpit floor structure, which included portions of the crew seats, sections of the instrument panel, and the nose tunnel structure with the nose gear assembly partially attached, had separated and rotated to the right and aft. This structure was in a partially inverted position.

Photo copyright Jeff Schroeder - used with permission
Of the 181 passengers and eight crew members aboard, eight passengers, the flight engineer, and a flight attendant were killed. There were 21 passengers and two crew members who were seriously injured. Although there were many occupied houses and apartment complexes in the immediate vicinity of the accident, there were no casualties outside the airplane.
All of those fatally injured during the crash were seated on the right side of the airplane between the flight engineer's station in the cockpit and row 5 in the passenger cabin. That section of the aircraft was destroyed during the accident sequence. The most seriously injured passengers were seated in the right forward portion of the cabin near an area of the fuselage which appeared to have been penetrated by a large tree. These persons were seated near those passengers who were injured fatally. Some seriously injured passengers were seated in the rear cabin near the trailing edge of the wings.
The fuselage in this area had been penetrated and the floor and seats had been disrupted.

Photo Copyright Robert Hockemeijer - used with permission
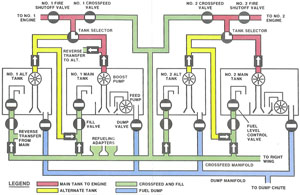
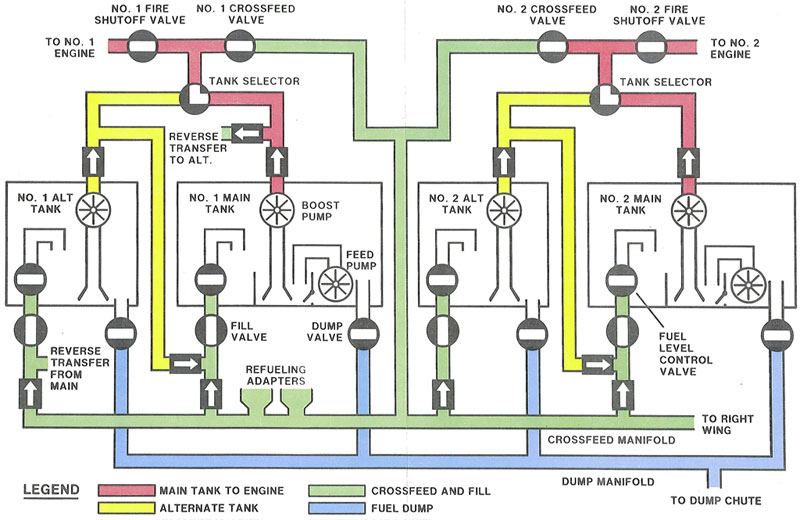
DC-8 Fuel System and Unusable Fuel
The DC-8-61 can be configured with a total of eight, nine, or ten fuel tanks. The total number of fuel tanks each aircraft has depends upon whether center auxiliary tank and/or wing leading edge auxiliary tanks are installed. The basic aircraft consists of eight tanks and each set of tanks (1-4) consists of a main and an alternate fuel tank. The normal operation of the aircraft would be that each set of main/alternate tanks feeds a specific engine. View a United Airlines training document containing a description of the fuel system.
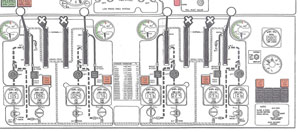
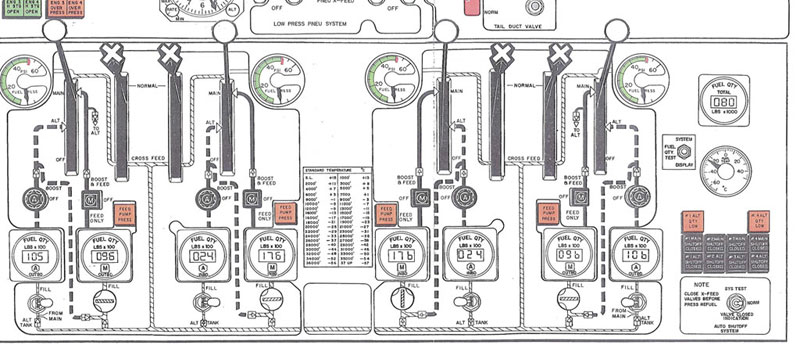
Fuel quantity remaining in each tank is provided to the flight crew by a set of gauges installed in the flight engineers panel.
View Large
{kind=link}
View Large
{kind=link}
A new type of fuel quantity indicating system was retrofitted to this aircraft on May 12, 1978. With the new system installed, there are eight individual tank quantity gauges. Each of these gauges has three digits. On these individual tank gauges, the digital reading is multiplied by 100 to obtain the total amount of fuel in the tank.
The totalizer gauge receives input from each individual tank gauge and displays the total fuel available on three digital readouts. However, this digital reading must be multiplied by 1,000 to obtain the value of the total amount of fuel on board. The smallest increment of change that can be indicated on the individual tank gages is 100 pounds. The smallest increment of change on the totalizer is 1,000 pounds.

The FAA certification standards required that aircraft fuel quantity gauges in the aircraft to be calibrated so that each gauge reads zero when all the useable fuel has been used from that tank. The amount of unusable fuel is established by flight tests to determine how much fuel is left in the tanks when the ports for the fuel pumps first become uncovered. The amount of fuel left in the tanks at this point is referred to as the unusable fuel and the fuel quantity gauges in the cockpit are calibrated to read zero, in level flight, when only the unusable fuel is left in a given fuel tank.
View the Unusable Fuel Animation below:
Flight Crew Coordination
The hierarchical "chain of command" system in place at the time of the accident did not always provide for effective flight crew resource management. This was evident to the investigation, as the second officer failed to adequately express the appropriate level of concern about fuel state of the aircraft. It was also clear in the accident report that the captain was not aware of the fuel remaining on board as he repeatedly asked "Why?" when informed that the first of the engines had flamed out.
Passenger Manifests
There was anecdotal information following the accident that some of the surviving passengers were able to find ground transportation (taxis) from the crash site to the airport and were later found waiting in the baggage claim area of PDX. As a result, their absence at the crash site reportedly made it difficult for emergency first responders to determine how many passengers had been on the airplane and how many had survived the accident.
As a result of this accident, the NTSB issued a recommendation to the FAA to "Include in the anticipated new rule a requirement for domestic and flag air carriers to maintain passenger lists with the provision that both ticketed and non-ticketed passengers' names be provided. This recommendation was subsequently adopted by the FAA.
The NTSB issued 15 findings, variously covering the events leading to the crash.
Further, the NTSB issued the following probable cause:
"The National Transportation Safety Board determined that the probable cause of the accident was the failure of the captain to monitor properly the aircraft's fuel state and to properly respond to the low fuel state and the crew-member's advisories regarding fuel state. This resulted in fuel exhaustion to all engine‘s. His inattention resulted from preoccupation with a landing gear malfunction and preparations for a possible landing emergency.
Contributing to the accident was the failure of the other two flight crewmembers either to fully comprehend the criticality of the fuel state or to successfully communicate their concern to the captain."

Photo copyright Jeff Schroeder - used with permission
The NTSB issued ten safety recommendations related to this accident. The recommendations covered a number of issues, most notably including flight crew training, review of aircraft certification criteria, and recommendations to audit related Supplemental Type Certificate approvals. The NTSB also included recommendations for regulatory change to require airlines to maintain passenger list for both ticketed and un-ticketed passengers.
The complete text of the recommendations is available at the following link: Accident Board Recommendations.
The DC-8 was originally certified per the requirements of Civil Air Regulations (CAR) 4b. Additionally, the STC which installed the fuel gages also used CAR4b.
The relevant CAR 4b regulations were:
CAR 4b.604 Powerplant Instruments, and
CAR 4b.613 Powerplant Instruments - Installation Requirements
Additionally, the following operational requirements are relevant:
14 CFR §91.3 - Preflight Action
"Responsibility and authority of the pilot in command.
(a) The pilot in command of an aircraft is directly responsible for, and is the final authority as to, the operation of that aircraft.
(b) In an in-flight emergency requiring immediate action, the pilot in command may deviate from any rule of this part to the extent required to meet that emergency.
(c) Each pilot in command who deviates from a rule under paragraph (b) of this section shall, upon the request of the Administrator, send a written report of that deviation to the Administrator."
14 CFR §121.557 - Emergencies: Domestic and Flag operations
"Emergencies: Domestic and flag operations.
(a) In an emergency situation that requires immediate decision and action the pilot in command may take any action that he considers necessary under the circumstances. In such a case he may deviate from prescribed operations procedures and methods, weather minimums, and this chapter, to the extent required in the interests of safety.
(b) In an emergency situation arising during flight that requires immediate decision and action by an aircraft dispatcher, and that is known to him, the aircraft dispatcher shall advise the pilot in command of the emergency, shall ascertain the decision of the pilot in command, and shall have the decision recorded. If the aircraft dispatcher cannot communicate with the pilot, he shall declare an emergency and take any action that he considers necessary under the circumstances.
(c) Whenever a pilot in command or dispatcher exercises emergency authority, he shall keep the appropriate ATC facility and dispatch centers fully informed of the progress of the flight. The person declaring the emergency shall send a written report of any deviation through the certificate holder's operations manager to the Administrator. A dispatcher shall send his report within 10 days after the date of the emergency, and a pilot in command shall send his report within 10 days after returning to his home base."
14 CFR §121.627 - Continuing flight in unsafe conditions
"Continuing flight in unsafe conditions.
(a) No pilot in command may allow a flight to continue toward any airport to which it has been dispatched or released if, in the opinion of the pilot in command or dispatcher (domestic and flag operations only), the flight cannot be completed safely; unless, in the opinion of the pilot in command, there is no safer procedure. In that event, continuation toward that airport is an emergency situation as set forth in section 121.557.
(b) If any instrument or item of equipment required under this chapter for the particular operation becomes inoperative en route, the pilot in command shall comply with the approved procedures for such an occurrence as specified in the certificate holder's manual."
14 CFR §121.639 - Fuel supply: All domestic operations
"Fuel supply: All domestic operations.
No person may dispatch or takeoff an airplane unless it has enough fuel-
(a) To fly to the airport to which it is dispatched.
(b) Thereafter, to fly to and land at the most distant alternate airport (where required) for the airport to which dispatched; and
(c) Thereafter, to fly for 45 minutes at normal cruising fuel consumption or, for certificate holders who are authorized to conduct day VFR operations in their operations specifications and who are operating non-transport category airplanes type certificated after December 31, 1964, to fly for 30 minutes at normal cruising fuel consumption for day VFR operations."
14 CFR §121.647 - Factors for computing fuel required
Factors for computing fuel required.
Each person computing fuel required for the purposes of this subpart shall
consider the following:
(a) Wind and other weather conditions forecast.
(b) Anticipated traffic delays.
(c) One instrument approach and possible missed approach at destination.
(d) Any other conditions that may delay landing of the aircraft.
For the purposes of this section, required fuel is in addition to unusable
fuel.
14 CFR §121.693(e) - Load Manifest: All certificate holders
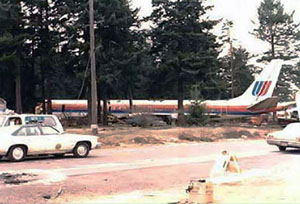
Photo copyright Jeff Schroeder - used with permission
The captain had significantly more overall flying time, as well as much more time in this type of aircraft, than either the first officer or the flight engineer. This may have made these subordinate crew members more likely to rely upon, and less likely to openly question, the captain's decisions.
At this point in commercial aviation history, a serial "chain of command" approach to cockpit resource management was more the norm than it is today. This also may have led to greater reliance on the captain's decision making. In any case, this accident played a pivotal role in identifying the need for a more parallel "team" approach to cockpit resource management as well as greater assertiveness on the part of subordinate crew members.
The hierarchal "chain of command" system in place at the time of the accident did not always provide for effective flight crew resource management. Additional training was identified as being needed to ensure the flight crews recognized the value and merits of flight crews breaking down the more formal hierarchal structure. This approach leads to a more participative and collaborative process to ensure that all members of the flight crew feel free to speak up and provide the captain with all relevant information relating to the safety of the aircraft.
The flight crew incorrectly assumed that additional fuel was still available even when the fuel tank quantity indicators read zero or nearly zero.
Eastern Air Lines Flight 401 was a Lockheed L-1011 jet that crashed into the Florida Everglades on the night of December 29, 1972, causing 101 fatalities (77 initial crash survivors, two died shortly afterward). The crash was a controlled flight into terrain as a result of the flight crew's failure to monitor the flight instruments during a malfunction of the landing gear position indicator system. While this crash was not the result of fuel starvation, this crash was similar to the Flight 173 crash as the crew of Flight 401 was occupied with a gear position light malfunction and did not properly monitor the flight path of the aircraft as it descended into the terrain.
See accident module
Section 121.693(e) was changed, effective August 31, 1980, to require the names of all passengers be maintained as part of the load manifest.
This accident, as well as the Eastern Airlines Flight 401 accident in 1972 was a catalyst for changes which resulted in the eventual adoption of CRM philosophies by many major carriers and, finally, by the FAA. CRM was first adopted in 1981 by United Airlines following a 1979 NASA workshop. Other airlines quickly followed suit. In 1990 the FAA initiated a voluntary "Advanced Qualification Program" (AQP), which included CRM training. CRM training has since become a regulatory requirement. A paper titled "The Evolution of Crew Resource Management Training in Commercial Aviation," written by a group at the University of Texas, explains the historical development of CRM training.
The most recent advisory material related to CRM (as of June 2007) is available at the following links: (newer versions may be created at any time)
Advisory Circular (AC) 120-51E, "Crew Resource Management Training," dated January 22, 2004
AC 120-71, "Standard Operating Practices for Flight Deck Crewmembers," dated December 13, 1991 - Part 1, Part 2
AC 60-22, Aeronautical Decision Making - Part 1, Part 2

Photo copyright Jeff Schroeder - used with permission
No Airworthiness Directives were issued as a result of this accident.
Airplane Life Cycle:
- Operational
Accident Threat Categories:
- Crew Resource Management
- Fuel Exhaustion
Groupings:
- Approach and Landing
Accident Common Themes:
- Human Error
Human Error
The hierarchal "chain of command" system in place at the time of the accident did not always provide for effective flight crew resource management. This accident, along with its precursors, resulted in the FAA's requirement for all air carriers to adopt CRM as an operational tool.
Eastern Air Lines Flight 401
Eastern Air Lines Flight 401 was a Lockheed l-1011 jet that crashed into the Florida Everglades on the night of December 29, 1972, causing 101 fatalities (77 initial crash survivors, two died shortly afterward). The crash was a controlled flight into terrain as a result of the flight crew's failure to monitor the flight instruments during a malfunction of the landing gear position indicator system.
See accident module
Technical Related Lessons
The risk associated with a flight crew's preoccupation with an emergency can exceed the risk posed by the emergency itself. (Threat Category: Crew Resource Management)
- During the course of the investigation, it became apparent that the flight crew did not keep track of the fuel onboard and the fuel flow rates. The crew had the fuel quantity information available to them to accurately determine their remaining flying time. However, this information was either overlooked or not effectively conveyed to the captain.
Common Theme Related Lessons
Crew Resource Management (CRM) training can enhance the ability to prevent and/or manage flight crew errors, and in maintaining continuity in flight crew performance of duties. (Threat Category: Human Error)
- During the investigation, it was found that only at one point did the flight engineer comment about the possibility of being low on fuel. However, no other information or details were provided to the captain who, even as the engines began to fail, believed they still had sufficient fuel on board to land the airplane.