
Eurocopter AS350B2
Air Tour / Commercial Operator
Juneau, Alaska
September 10, 1999

On September 10, 1999, three Eurocopter AS350B2 helicopters crashed within five hours and two miles of each other near Juneau, Alaska. There were no fatalities from any of these accidents. All three aircraft were operated by the same certificate holder. The three flights originated in Visual Meteorological Conditions (VMC) operating under Visual Flight Rules (VFR). The first aircraft was operating as a 14 CFR Part 135 air tour company. The second and third aircraft were operating under 14 CFR Part 91. The pilots of all three aircraft experienced spatial disorientation.
The National Transportation Safety Board (NTSB) determined the probable cause of the first accident was the pilot’s continued flight into Inadvertent Instrument Meteorological Conditions (IIMC) and inadequate altitude and clearance. Factors associated with this accident were flat light, whiteout conditions, snow, and snow-covered terrain. The probable cause for the second and third accidents were the pilots' failure to maintain altitude and clearance. Factors associated with the second and third accidents were flat light conditions, snow-covered terrain, and self-induced pressure to continue the search for the first accident aircraft.
NTSB accident reports: ANC99FA139, ANC99LA140, and ANC99LA141
History of Flight

On September 10, 1999 at 1204 local time, an Eurocopter AS350B2 helicopter (Accident Aircraft #1) with a pilot and five passengers onboard departed Juneau, Alaska Airport on a VFR 14 CFR Part 135 air tour flight to the Juneau Icefield. After departing the glacier to return back to Juneau Airport, the pilot encountered IIMC. When all external visual cues were lost, the pilot became spatially disoriented and the aircraft impacted the terrain. The pilot and five passengers survived, with one sustaining serious injuries and the remaining receiving minor injuries. The aircraft came to rest in a nearly inverted attitude and was destroyed in the accident.
Aircraft #1 was the first of three Eurocopter AS350B2 helicopters owned by the same operator that crashed that day. Accident Aircraft #2 and Accident Aircraft #3 began to search for the missing aircraft. Later, the United States Coast Guard (USCG), with their HH-60 Jayhawk helicopter, began its search and rescue operations.
The operator’s base manager took a helicopter to conduct a search for Aircraft #1. This decision resulted in no operational oversight at the base. Without coordinating with management, the flight crew of Aircraft #2 made a hurried decision to depart Juneau airport at 1345 local time as a VFR 14 CFR Part 91 flight to also search for overdue Aircraft #1.
Another company pilot was aboard Aircraft #2 as an observer. He said the horizon was visible for 50 miles with a ceiling of 1,000 feet that descended to 500 feet as the flight progressed. He was using binoculars and estimated the altitude as 500 feet above the ground at the time. The terrain directly beneath the helicopter was almost impossible to evaluate due to the flat light conditions present. There was gradually rising terrain in the area, with some topography that protruded upwards.

As the crew encountered these atmospheric conditions, the pilot experienced spatial disorientation, began to slow the aircraft speed, and was unable to correctly determine the aircraft altitude above the terrain. Aircraft #2 impacted the surface of the ice field at approximately 1445 and sustained substantial damage. Both the pilot and passenger survived.
At 1530, Aircraft #3 was on a VFR 14 CFR Part 91 flight en route to the Juneau airport when it was informed of missing Aircraft #1. The helicopter was being flown by one of the operator’s more experienced pilots with a front seat passenger who was also pilot certificated. Aircraft #3 was told to return to the Juneau airport as planned. However, Aircraft #3 elected to assist in the search for the first accident aircraft instead of returning to Juneau.
While conducting the search, the crew received a radio call from the pilot of recently crashed Aircraft #2 requesting assistance. Worsening weather prevented immediate rescue, so Aircraft #3 returned to the Juneau airport to refuel and wait for better conditions. Once the weather improved, Aircraft #3 returned to the area of the accident sites and found Aircraft #2. At that point, the environmental conditions had not improved. The observer estimated the weather conditions as being among the worst he had ever seen. Aircraft #3 was able to land and pick up the two Aircraft #2 crewmembers. It was then agreed by both crews to return directly to the airport.
With four persons now on board, Aircraft #3 took off. As they began their departure, another helicopter operating for a different company made a radio call on a common frequency with location information for the accident site of Aircraft #1. The four pilot-certificated occupants aboard Aircraft #3 decided to search for Aircraft #1 before heading back to the airport. While climbing to altitude, they spotted the crash site of Aircraft #1. After a short discussion, the persons onboard Aircraft #3 unanimously agreed to land and assess the situation at Aircraft #1.
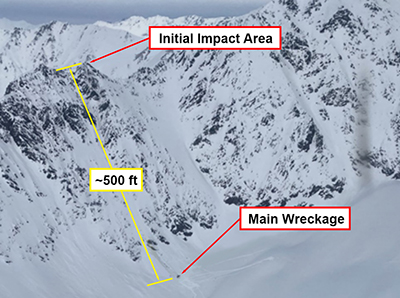
The flat light conditions made it difficult to determine the altitude of the helicopter above the ground. The crew was estimating that they were 500 feet above the surface, and the pilot assigned the front seat passenger to advise him if the aircraft descended below 5,200 feet Mean Sea Level (MSL). As the aircraft descended through 5,200 feet to about 5,150 feet, one of the rear passengers was about to alert the pilot of the altitude deviation. Before the warning was made, Aircraft #3 struck the snow-covered ice field, causing substantial damage to the helicopter. The four individuals were not seriously injured.
The NTSB commented that there were observable skid marks stretching back about 300 feet from the impact site of Aircraft #3. The people aboard Aircraft #3 were not aware they were skimming along the ground for hundreds of feet until they crashed.

Hours after the first aircraft accident occurred, a USCG HH-60 Jayhawk helicopter was dispatched and arrived on scene to attempt the rescue. The crew was unable to land at the accident sites due to deteriorating weather conditions. They instead landed a few miles away to a more favorable location which allowed them to drop off a search and rescue ground team who hiked to the location of the crash victims. As a result of the weather conditions, all ten personnel from the three helicopters were forced to remain on the Juneau Icefield overnight.
The following day, the USCG helicopter was able to reach the people stranded by these three accidents. Upon arrival at the accident scene of Aircraft #1, the USCG rescue crew assessed the snow-covered terrain. The area did not appear stable enough to attempt a landing since the aircraft was not equipped with landing gear skis.
The flight crew discussed how to mitigate potential hazards, such as a sudden whiteout condition in an area where they were unable to land. The flight crew took safety measures that included saving a GPS waypoint of a precipice with a 300-foot drop-off noted on their inbound flight so they could return to a place of safety if a whiteout occurred.
The flight crew eventually determined the best recovery option was to hover over the crash victims and use a hoist to bring them aboard. As the last passenger was secured in the aircraft, the Jayhawk became enveloped in a rapidly developing snow shower. Witnesses at the third crash site observed the snow obscure the helicopter, which had personnel still on the hoist, and noted the aircraft made sudden, excessive pitch and bank angles.
Almost immediately afterwards, they observed multiple items being tossed off the aircraft. Once enveloped in the snow, the Coast Guard crew used "Altitude Hold" automation to assist them in maintaining ground clearance. Using the tossed items as visual reference points, the crew slowly backtracked to the GPS point marking the 300-foot drop off. Upon arrival at the point, the Jayhawk was able to descend from the poor visibility back into a VMC environment. Subsequently, all persons were successfully flown to the Juneau airport.
Flight Into Degraded Visual Environments
The pilots in these three accidents were flying in flat lighting conditions. Flat light is a subset of atmospheric hazards commonly described as Degraded Visual Environments (DVE). The height above the terrain was not accurately determined because of obscurants, lighting, or poor surface contrast. DVE can make it difficult or impossible for pilots to maintain visual reference with the ground or horizon. DVE induces a condition of limited visibility to outside references in varying degrees which can lead to lack of situational awareness and loss of aircraft control.
Certain geographic areas require special training to minimize risks from frequently occurring DVE. Pilots must be aware of DVE conditions and know how to recognize, avoid, and escape them. Areas with airborne particulates and low contrast terrain require special vigilance to recognize and safely navigate. DVE is most common in geographic areas with a potential for flat light, whiteout, or brownout conditions, such as deserts, snow, or ice fields. The following describes some of the DVE conditions that helicopter pilots may encounter:



Flat Light – Also known as sector or partial white out, a flat light environment reduces the amount of visual contrast to the point that the horizon is indistinguishable from the terrain. It is more insidious than a complete whiteout condition because pilots may not notice the gradual loss in the contrast and depth-of-field cues until all usable ground references are lost. Flat light is usually accompanied by overcast skies and often occurs in snow covered areas, but can occur in dust, sand, mud flats, or on glassy water. Flat light can completely obscure features of the terrain, creating an inability to distinguish distances and closure rates. As a result of this reflected light, it can give pilots the illusion of ascending or descending when actually flying level.
Whiteout – As defined in meteorological terms, whiteout is when a person becomes engulfed in a uniformly white glow. The glow is a result of being surrounded by blowing snow or water. There are no shadows, no horizon or clouds, and all depth-of-field and orientation cues are lost. A whiteout situation is hazardous because of the complete loss of visual references. Flying is not recommended in any whiteout situation.
Flat light conditions can lead to a whiteout environment quite rapidly, and both atmospheric conditions reduce visual references slowly until they may disappear completely. Some pilots have caused self-induced whiteouts. This effect typically occurs when a helicopter takes off or lands on a snow-covered area. The rotor downwash picks up snow and re-circulates it through the rotor system, in effect creating a cloud that obscures the pilot’s vision. The effect can vary in intensity depending upon the amount of light on the surface. This phenomenon can happen on the sunniest, brightest day with good contrast everywhere. However, when it happens, there can be a complete loss of visual cues.
Brownout – Helicopter brownout is similar to whiteout, but often occurs during takeoff or landing in dusty environments. Sand or dust is swept up in the rotor outwash and obscures the pilot's vision of the terrain. This is particularly dangerous because the pilot needs visual cues from their surroundings to make a safe landing.
If a pilot encounters a DVE situation, quick action is needed to fly out of the area safely. If the aircraft is properly equipped, the pilot must immediately transition to instrument flight when VMC is lost. Responding to an IIMC event is now a flight check requirement for 14 CFR Part 135 operations. However, at the time of these accidents, it was not a Part 135 requirement.
If a pilot is unable to transition to instrument flight, it is possible to increase the visual contrast of an environment by strategically dropping things from the aircraft. Brightly colored items placed on a low-contrast surface provides visual references for landing or hovering purposes. A single reference point can be obscured or disappear as the aircraft attempts to land or depart the area visually.
Radar altimeters provide useful information, but this data is limited to what is directly beneath the aircraft at that moment. Terrain or obstacles in front or behind may not be at the same height as the terrain underneath the aircraft. Additionally, some surfaces may provide erroneous feedback, giving incorrect altitudes to the pilot.
In low contrast situations, automation such as "altitude hold" or "hover hold" should be used when available.
Storing GPS waypoints of the lowest terrain in the immediate area, such as was done by the USCG air crew during this rescue, can help guide an aircraft to the safest area for recovery or for extended hover operations while waiting for conditions to improve.
Pilot Decision Making
Pilot decision making played a role in all three of these accidents. DVE had not been formally developed as a training requirement, and the pilots did not recognize how suddenly or drastically it could affect flying conditions. The lack of knowledge on how detrimental this critical weather phenomena may be played a significant role in the accident pilots’ decision-making process. Subsequent interviews with personnel that were present and familiar with these accidents provided crucial details to help determine probable human factors in the decision-making. According to investigators, it is likely that decisions made by the base manager, an experienced pilot, as well as decisions made by base dispatch personnel played a role in at least one of the accidents.
The pilot flying Aircraft #1 was faced with worsening weather as he continued to the airport. Self-imposed pressures urged him to complete the flight. Options such as returning to the point of departure or landing immediately to wait for better weather were available but not chosen. Plan continuation bias (a form of confirmation bias also known as "get-there-itis"), expectation bias, and organizational pressures may have led him to believe the flight could be completed with the original plan.
The pilots aboard Aircraft #2 were affected by time pressure. Time pressure drove the pilots to launch and help with the search. In their rush, they failed to ensure the upper management team was notified of their plan to look for Aircraft #1. The July 2023 issue of CALLBACK published by NASA addressed time pressure, stating "Time pressure is complex. It has influence on quality of decisions, and it rarely acts alone, but rather in concert with other human factors. Events can suddenly thrust a pilot or crew unwittingly into a continuum where decisions must be made in minimal time. A good decision may reduce pressure, advance clearer thinking, and effect better results. A lesser decision could cause or increase pressure and may further jeopardize judgment and the safest course of action."
The crew felt an urgent need to locate Aircraft #1 before night fell and temperatures plummeted. This sense of urgency led to impulsivity, the need to do something right away. Impulsivity is one of the five "Hazardous Attitudes" outlined in Chapter 2 of the Pilot Handbook of Aeronautical Knowledge (PHAK).
Effective company procedures can reduce the number of hurried decisions made by front-line employees and reduce errors caused by time pressure. Conversely, a lack of good procedures can place additional pressures on front-line employees, increasing hazards and risks.
Other organizational pressures also affected the crew aboard Aircraft #2. The flight dispatch department at the Juneau base had not notified anyone outside of the base of the overdue Aircraft #1. No one in upper management of the certificate holder’s organization was aware of this event, and government emergency and search and rescue organizations were not notified until more than 90 minutes after the first aircraft had crashed.
One of the aircrew involved in this series of accidents stated that upper management would have grounded all subsequent flights if they had been notified of the first missing aircraft. The hasty launch of the second aircraft may have been prevented.
A second organizational pressure was caused by the absence of the base manager. He had launched out in yet another aircraft to search for the missing first aircraft. If the base manager had remained at the airport, it is likely that the dispatch team at the base would have notified the certificate holder senior management and appropriate government organizations in a timely manner.
Those aboard Aircraft #3 were affected by the same time pressure, and subject to the same impulsivity hazards as the crew of Aircraft #2. The Aircraft #3 pilot knew his experience in the local area gave him the best chance of finding the missing aircraft. He too recognized the approach of night and its associated plummeting temperatures as a risk to human life. This influenced the decision to attempt a rescue.
Human Factors and Decision Making
Effective decision-making is optimized when people have the necessary data and time for thoughtful analysis. An organization developing a procedures manual has the time and resources to consider complex, foreseeable contingencies and develop appropriate planned responses. In emergency situations, pilots and operations personnel often have limited time and data to develop well-thought out decisions. Biases based on previous experience may expedite their decision-making. Unfortunately, decisions influenced by pressures and biases do not always lead to desirable outcomes. Properly developed and implemented procedures can reduce the need for ad-hoc decisions made on the flightline and in the cockpit.
The FAA has identified a list of common causes of mistakes related to human factors that can result in accidents, called the "Dirty Dozen." Pressure is one of the Dirty Dozen, and it can be a real or perceived force demanding high-level performance. Pressures affecting decisions can be external, internal, or a combination of both.
According to the PAVE Checklist, "External pressures are influences external to the flight that create a sense of pressure to complete the flight." These pressures can come from influences outside the employees control, such as organizational culture and expectations or bad weather. An expected minimum number of revenue operations per day or per employee is an example of an external pressure created by the organization.
Internal pressures are self-imposed by the individual, as discussed in Aviation Safety Magazine, "Feeling the Pressure." Lack of preparation can be an example of internal pressure. A choice to leave behind a rarely used (but useful) piece of equipment, such as a jacket, or a hand-held radio, could cause pilots to make riskier decisions when unexpected situations arise. Time pressure can be an example of internal pressure: the employee may have given others an expected timeline, and unexpected delays can cause increased pressure and stress. Shortcuts may be taken to try and get back on the timeline.
Sometimes pressure is more complex, with both internal and external characteristics. The rapidly deteriorating Arctic winter weather associated with the mishap of Aircraft #1 placed complex time pressure on the crews of Aircraft #2 and Aircraft #3. The decision making that resulted was based off an external event to the crews, but also placed internal pressure on them to do something.
Biases result from the human’s attempt to simplify information and speed up problem solving. They are mental shortcuts used to aid in decision making. There are two broad categories of bias: expectation bias and confirmation bias. Expectation bias is a strong belief or mindset towards something we expect to see or hear, and actions taken according to those beliefs. Confirmation bias is seeking out data to confirm preconceptions. Biases can be helpful when quick decisions need to be made, but they also pose significant risk. "Sometimes...biases lead to poor decisions and bad judgements. The most important tool to countering biases is to know they exist, and to understand when you might be most susceptible." (FAA Safety Briefing, June 30, 2020.)
Individual decision making is subject to errors from biases and pressures. These can be reduced by having prepared responses or procedures in place. Organizational influences (procedures and management) are the first lines of defense to prevent potential accidents. Human error has been identified as a factor in two-thirds to three-fourths of aviation accidents and incidents. By emphasizing human factors in operational planning and procedures, the number of human error-related mishaps will likely be reduced. The Role of Human Factors in the FAA.
Conclusion
The accident of Aircraft #1 was the catalyst that led to the mishaps of Aircraft #2 and Aircraft #3. The absence of operational controls led to downstream pressures. A lack of clearly written procedures allowed the crews of Aircraft #2 and Aircraft #3 to make their own decisions to participate in the search effort. The operator's pilots conducting the search operations determined it was necessary to fly into the unknown and extremely hazardous environmental conditions, and they had no requirements to notify the management of their plans to do so.
The informal DVE and spatial disorientation training given to company aircrew did not adequately prepare them for the encountered situation. These pilots were not properly prepared and the aircraft were not properly equipped to conduct this search safely or successfully. Without clearly established procedures and approval processes in place, the crews of Aircraft #2 and Aircraft #3 did not adequately determine the risks associated with the search, ultimately leading to their accidents.
The USCG aircrews also felt immense pressure to rescue the stranded victims. Lifesaving is a critical Coast Guard mission. Improper or hurried decisions could easily lead to a mishap. To maximize the probability of success in such demanding circumstances, the USCG used a wide range of tools and operational controls to reduce risk. Intense and formal aircrew training, highly specialized equipment, and repetitive experience in similar environments provided them the needed edge to rescue those lost in bad weather.
The National Transportation Safety Board determined the probable causes of this accident to be the pilot’s continued flight into instrument meteorological conditions (IMC) and inadequate altitude/clearance. Factors associated with the accident were flat light and whiteout conditions, snow, and snow-covered terrain. An additional factor was the FAA's inadequate certification/approval of the operator's training manual, which did not require the operator to provide instrument training or instrument flight checks to its pilots.
Findings from the three NTSB accident reports are summarized as follows:
Aircraft #1 - Continued flight into IIMC, resulting in spatial disorientation and an aircraft accident.
Aircraft #2 - Failure to maintain altitude with flat light conditions, fog, and snow-covered (low-contrast) terrain, resulting in spatial disorientation and an aircraft accident.
Aircraft #3 - Failure to maintain altitude with flat light conditions, snow-covered (low-contrast) terrain present, resulting in spatial disorientation and an aircraft accident. An additional finding was self-induced pressure to continue the search.
NTSB accident reports: ANC99FA139, ANC99LA140, and ANC99LA141
14 CFR Part135.23(d) - Manual Contents – Certificate holders must have procedures for complying with accident notification requirements. These procedures appear to have been non-existent, ineffectively written, or ineffectively utilized by the certificate holder when Aircraft #1 was noted as missing by the flight operations at Juneau airport.
14 CFR Part 135.79(a)(2) - Flight Locating Requirements – Certificate holders must have procedures established for locating each flight for which an FAA flight plan has been filed, and provide for timely notification to an FAA or search and rescue facility if an aircraft is overdue or missing. This procedure appears to have been non-existent, ineffectively written, or ineffectively utilized by the certificate holder when Aircraft #1 was noted as missing by the flight operations at Juneau airport.
14 CFR Part 119.69(d)(3) - Management personnel required for operations conducted under part 135 of this chapter – Personnel assigned operational control must discharge their duties to meet applicable legal requirement and maintain safe operations. The Juneau base flight operations and management team failed to ensure regulatory requirements were met regarding the proper reporting of overdue aircraft, missing aircraft, or aircraft accidents, demonstrating an apparent lack of compliance.
14 CFR Part 119.5(g) - Certifications, authorizations, and prohibitions – No person may operate as a direct air carrier or as a commercial operator without, or in violation of, an appropriate certificate and operations specifications.
14 CFR Part 135.21(a) - Manual Requirements – Certificate holders must have and keep current a manual with policies for use during flight, ground, and maintenance operations. The inability of base personnel to contact agencies outside of the Juneau airport identified a significant shortcoming in the company published policies and procedures.
The certificate holder did not provide adequate operational control over the
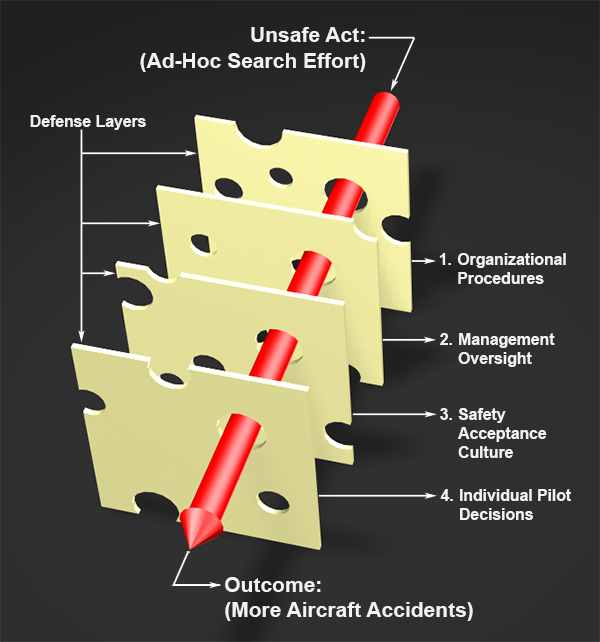
flights. The prevailing weather should have stopped operations for the day. Organizational procedures, management oversight, and a good safety culture within the company should have provided layers of defense to mitigate the risks created from individual decisions. Lacking these safeguards, individual decisions led to this series of accidents.
Reason's Model of Accident Causation applied to the accidents of Aircraft #2 and Aircraft #3
- No organizational documents outlining accident/overdue aircraft procedures
- Manager left no clear guidance or expectations prior to conducting his own search
- Safety culture should have given operations personnel the ability to notify outside agencies of missing aircraft or other emergencies
- Other pilots followed the manager's lead to find and rescue missing aircraft in inclement weather
Lack of operational controls – Upper management was not notified of missing Aircraft #1 and other pilots were allowed to fly subsequent aircraft without formal approval processes or direct management oversight.
DVE operations risk – Sudden meteorological changes, such as flat light or whiteout conditions, can dramatically reduce the visibility needed for pilots to safely operate under VFR.
Insufficient training and evaluation – Pilots were trained and evaluated to perform their flights under VFR but did not have any IIMC training or evaluations documented.
Organizational pressures and self-imposed pressures – Specific examples of how these pressures impacted the decisions made by the crews of Aircraft #2 and Aircraft #3 are listed below.
Organizational Pressure – Lack of oversight. The base manager left no one in charge when he took a helicopter out to search for the overdue aircraft. No guidance was provided for the employees in his absence. Once he departed the airport, subsequent decisions were placed solely on the front-line employees.
Organizational Pressure – Failure to establish or follow written procedures. The organization’s lack of established procedures delayed the missing aircraft notification to company senior management and professional rescue agencies. This delay and subsequent lack of response prevented upper management from taking control of the situation. This placed the pressure of the search effort directly on the front-line employees and led to individual decision-making errors.
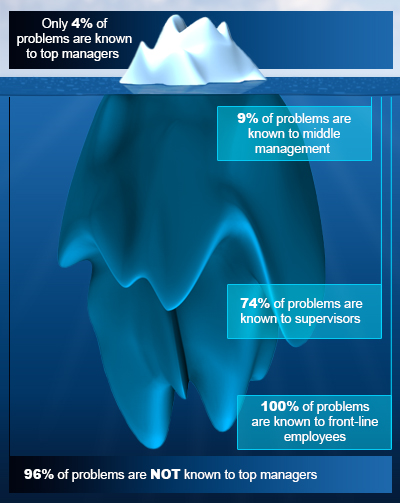
Organizational Pressure – Poor Safety Culture. The reluctance of flight operations personnel to contact anyone without prior approval from the base manager indicates the organization had a poor safety culture. A good safety culture is open and non-punitive. Employees can report problems or mistakes without risking their jobs. Companies with strong safety cultures encourage reporting and are more likely to find the root causes of systemic problems before they become incidents or accidents.
Self-Imposed Pressure – Expectation Bias. The pilot of Aircraft #1 had just completed a relatively short flight in good weather and expected the weather for the return trip to be good since there were no obvious signs of change.
Self-Imposed Pressure – Expectation Bias. The base manager took an aircraft out to look for the overdue helicopter. Other employees saw this as the expectation and believed they should follow his lead and do the same thing.
Self-Imposed Pressure – Confirmation Bias. The pilots of Aircraft #2 and #3 expected to see weather that was safe for the search. Some visual cues confirming this bias were accepted, and other visual cues contradicting this bias were filtered out. The fact they could see distant mountain ranges out some windows overrode the degraded visibility seen nearer the aircraft.
In day, VMC flight, helicopter pilots can recognize worsening weather and land before losing visual reference with the ground.
- For Aircraft #1, the pilot encountered IIMC and was unable to determine his location relative to the terrain below the aircraft. A safe landing was impossible to conduct when outside references to the ground were not visible.
- For Aircraft #2 and #3, the pilots encountered DVE conditions (flat light) that allowed them to see the terrain beneath but prevented either one from determining the aircraft’s actual height above ground level. In this case, a safe landing could not be conducted because the pilots failed to recognize the aircraft's lower-than-expected height above the ground. The aircraft impacted the terrain as the pilots were expecting to be a few hundred feet above the ground.
A company's operational procedures provide all required information necessary for the safe conduct of flight activities.
- Limited to no communication was provided by management regarding search and rescue operations for Aircraft #1.
- When the base manager left in a helicopter to search for Aircraft #1, other pilots assumed that he was setting the best example of expectations to follow his direction and support the search.
- Certificate holders must have controls and procedures that clearly document how employees should respond in emergency situations.
Eurocopter AS-350BA, N6099S, Herbert Glacier near Juneau, AK, June 9, 1999
During this air tour flight, the pilot and six passengers were fatally injured after departing for a 50-minute flight over mountainous glaciers. About ten minutes after a normal radio transmission, the wreckage from this helicopter was found by a pilot from a second helicopter company. The pilots of the only two helicopters near the accident scene at the time of the accident said the flat light made the featureless snow-covered terrain difficult to discern from the indefinite, overcast ceiling. The accident pilot did not have, and was not required to have, an instrument rating or any emergency instrument training from the company. The pilot had expressed to a previous employer and to a previous instructor that he was uncomfortable with company pressure to fly tours in bad weather.
NTSB accident report: ANC99FA073
Eurocopter AS-350B2, N197EH, Girdwood, AK, March 17, 1999
The accident helicopter was transporting skiers to a remote area that had recently received six inches of very light, powder snow. As the pilot was returning to pick up the next group of skiers, he hovered toward the landing area and became disoriented in whiteout conditions due to the blowing snow. He said the helicopter drifted to the right and the right side landing skid struck the snow. The helicopter rolled onto its right side and sustained damage to the fuselage, tail boom, and drive train components.
NTSB accident report: ANC99LA036
Bell 206 II, N371EH, Valdez, AK, April 28, 1992
After landing short of the intended destination due to poor weather, the pilot surveyed the area and elected to take off again. During the takeoff sequence, whiteout conditions caused him to abort and the aircraft touched down sooner than expected. Uncertain of the suitability of the terrain beneath the helicopter, he began to hover taxi back to the original takeoff point. During the taxi, he lost visual references due to whiteout conditions. The helicopter drifted to the right, and the right side landing skid struck a small hill. The aircraft rolled over and suffered substantial damage.
NTSB accident report: ANC92LA065
AS-350BA, N594BK, Mt. Waialeale, HI, June 25, 1998
While operating an aerial sight-seeing tour, the helicopter pilot encountered poor weather and the aircraft impacted an 80-degree upsloping face of a mountain 200 feet below its ridge crest. Three helicopters departed on the tour, with approximately two minutes between departures. The accident helicopter was the third of the three aircraft. The three aircraft remained in radio contact with each other throughout the flight. The company’s chief pilot was flying the first of the three aircraft. The second pilot relayed that he encountered heavy rain showers and lower visibilities near what would become the accident site. The accident pilot attempted to fly the same route as the previous two aircraft. The pilot became disoriented and transmitted to the pilots ahead of him the weather was getting worse and that he could not see. The helicopter impacted the terrain and all six aboard were killed. The NTSB determined the probable cause to be continued flight into deteriorating weather conditions. Another cited factor was the chief pilot’s failure to direct the following pilots to avoid the areas with known deteriorating weather.
NTSB accident report: LAX98FA211
Several safety initiatives resulted from this series of accidents.
The Certificate Holder
Operational and training changes were incorporated, including instrument competency checks and flat light conditions training for aircrew.
Radar altimeters have been installed for air tour helicopters operating over snow-covered glacial terrain. Emergency Locator Transmitters (ELTs) have been moved to the passenger cabin, and handheld radios have been provided for each helicopter.
NTSB
The NTSB included this series of accidents in a Safety Recommendation regarding the hazards of flat light to the FAA. This recommendation proposed additional training and checking requirements for pilots, as well as the addition of radar altimeters to helicopters.
FAA
14 CFR Part 135.293(a) was updated, mandating competency checks include an oral evaluation on flat light/whiteout/brownout topics.
14 CFR 135.293(c) was implemented, requiring basic instrument evaluations during pilot competency checks.
14 CFR 135.160 was created, requiring the use of radar altimeters in commercial helicopter operations.
Detailed information on flat light has been added to the Aeronautical Information Manual.
Rotorcraft Life Cycle
- Operational
Accident Threats
- Controlled Flight Into or Toward Terrain (CFIT)
- Low Altitude Operations (LALT)
- Unintended Flight in IMC (UIMC)
Operations
- Air Tour / Sightseeing
Accident Common Themes
- Organizational Lapses
- Human Error
- Flawed Assumptions
Organizational Lapses
The operator did not have, or did not adequately train, procedures for overdue or missing aircraft. The base manager was expected to give guidance to operations personnel in the event of an emergency. The manager failed to provide adequate instructions before taking another aircraft to search for the missing helicopter. Operations personnel did not contact outside rescue agencies until a supervisor outside the operator's organization arrived on scene and directed them to do so.
Human Error
The operator failed to provide operational controls through established procedures and relied on the ad-hoc decision-making of front-line employees to mitigate risks. In the absence of controls, improper individual decision-making occurred multiple times, leading to the mishaps of Aircraft #2 and #3.
Flawed Assumptions
When the base manager left in an aircraft to search for the missing helicopter, other pilots assumed that he was setting an example of expectations to follow and hastily launched in other aircraft without further coordination.
S-76A++, N579EH, Galveston, TX, March 23, 2004
While conducting a part 135 flight under visual flight rules transporting eight oil service personnel to a drilling ship 180 miles south of Galveston, Texas, the helicopter descended for unknown reasons and impacted terrain. The two pilots and eight passengers were fatally injured. The helicopter departed for its overwater flight eleven minutes before the end of evening civil twilight, and there was an overcast cloud layer at 4,000 feet. Eight percent of the moon disk was illuminated at the time of the accident. The NTSB determined the probable cause was the flight crew’s failure to identify and arrest the helicopters descent, which resulted in controlled flight into terrain. Safety issues in the NTSB report include a focus on terrain awareness and warning systems for helicopters.
NTSB accident report: AAR-06/02
AS-350, N194EH, Juneau, AK, May 5, 2016

While conducting a cargo flight in visual flight rules, the instrument rated pilot conducted an approach to a remote dog camp situated on a glacier. During the approach, the helicopter impacted terrain, coming to rest about three quarters of a mile away from the dog camp. The pilot reported flat light conditions were present during the approach. It is likely that the pilot failed to maintain terrain clearance due to his inability to distinguish distances and closure rates because of the flat light optical illusion.
NTSB accident report: ANC16LA022
AS-350B3, N351SH, Palmer, AK, March 27, 2021
A helicopter carrying passengers from a private residence to a heli-ski area at a nearby mountain attempted to land on a ridgeline. The pilot and four passengers were fatally injured when the helicopter impacted terrain. The surviving passenger stated the first approach was aborted, and the pilot lifted off for an attempted second landing. During this attempt, the passenger stated the helicopter became "engulfed in a fog which made it appear like a little white room." The helicopter subsequently began "going backward real fast." The pilot likely experienced whiteout conditions, losing visual reference with the ridgeline. The helicopter impacted the terrain and rolled back down the mountain.
NTSB accident report: WPR21FA143
AS-350BA, N99676, Valdez, AK, March 15, 2022

A helicopter being used to transport skiers inadvertently collided with terrain while maneuvering to land on a glacier. The pilot stated that while on an approach to pick up a group of skiers, flat light conditions made it difficult to make out topographical features on the snow-covered glacial terrain. The helicopter inadvertently descended below the approach path and touched down short of the intended landing site. After impacting the terrain, it rolled to the left and sustained damage to the main rotor blades, tail rotor blades, tail boom, and fuselage. The NTSB determined probable cause was the pilot’s failure to maintain a proper approach path in flat light conditions, resulting in landing short of the intended spot and impacting the terrain.
NTSB accident report: ANC22LA023
Technical Related Lesson(s)
Aircraft approved for single pilot operations and aircraft only approved for VFR operations should not attempt rescue missions when Degraded Visual Environments (DVE) conditions exist. (Threat Category: Low Altitude Operation, IIMC)
- Large aircraft certified for Instrument Flight Rules (IFR) require a crew of two pilots and are usually equipped with flight assist automation and other advanced systems designed to help mitigate the risks associated with DVE.
- Pilots authorized to fly large, IFR-certified aircraft receive specialized, documented training including operations in IMC conditions.
- IFR-certified aircraft approved for single pilot operations often do not have the appropriate automation or the requisite training requirements to minimize the risk in DVE rescue operations.
- The AS350B aircraft in this series of accidents were only certified for VFR operations. These aircraft were not equipped with the appropriate equipment to perform rescue operations in DVE conditions.
Before operating in DVE, pilots should receive specialized training and evaluations for recognition, avoidance, and recovery procedures. (Threat Category: Low Altitude Operation, IIMC)
- Brownout, whiteout, and flat light conditions are three subsets of DVE that can occur quickly and unexpectedly, producing extremely hazardous conditions for visual flight.
- The accident aircraft were flown by pilots who did not have adequate training on DVE topics by an approved training program, nor was it required at the time of the accidents.
- The pilots did not have appropriate IIMC training or evaluations documented in the company records, nor were they required at the time of the accidents.
Situational awareness enhancing equipment (e.g., radar altimeters, synthetic vision systems) and techniques should be used to improve flight safety in DVE-prone areas. (Threat Category: Low Altitude Operation)
- Situational awareness is critical for safe operations in DVE. Aircraft operating in these areas should take advantage of technology and tools to enhance situational awareness to escape a degraded environment.
- The accident aircraft did not have radar altimeters installed, nor were they required at the time of the accidents.
- Techniques (e.g., preplanning alternate routes, storing GPS waypoints, dropping high-contrast objects, etc.) can aid in escaping a DVE situation.
- In this series of accidents, the USCG helicopter was equipped with systems designed to enhance safety in adverse environments. A radar altimeter, flight assist automation (including altitude and attitude hold), and a GPS unit allowing easy “on the fly” storage of local waypoints all provided critical assistance in a visually degraded environment.
Common Theme Related Lesson
14 CFR Part 135 certificate holders should provide adequate operational oversight of flights. Clearly established procedures provide a defense barrier that can reduce or eliminate errors caused by individual decision making. (Common Theme: Organizational Lapse)
- Certificate holders should have well-developed processes for approving, dispatching, and modifying aircraft flights.
- There was a noted lack of flight operations management oversight in Juneau on the day of the three aircraft accidents.
- The certificate holder approval processes for dispatch or re-tasking of aircraft for a search and rescue operation was inadequate or non-existent.
- Notification to government officials such as police and USCG search and rescue assets were delayed by inefficient or non-existent reporting processes.
- The certificate holder did not provide adequate oversight of its flight operations. More effective management could have prevented the accidents of Aircraft #2 and Aircraft #3 and could have reduced the time Aircraft #1 spent waiting on rescue.
- Flight operations employees should be trained to immediately report mishaps to the certificate holder's upper management.
- A procedures manual emphasizing a positive "Safety Culture" could have empowered flight operations personnel to reach out to outside rescue organizations without first seeking management approval. When left without direct oversight, these employees felt they were not authorized to tell anyone of the missing aircraft. They did not notify anyone until another manager arrived at the base.