
Embraer EMB-120RT

Photo copyright Adriaan Lengkeek - used with permission
Continental Express Flight 2574, N33701
Eagle Lake, Texas
September 11, 1991
Continental Express Flight 2574 broke up in flight during descent. The horizontal stabilizer, or top of the T-type tail, had separated from the fuselage before ground impact. Examination revealed that the 47 screw fasteners that would have attached the upper surface of the leading edge assembly for the left side of the horizontal stabilizer were missing. These fasteners had been removed the night before during scheduled maintenance. The National Transportation Safety Board (NTSB) determined that the probable cause of the accident was the failure of Continental Express maintenance and inspection personnel to adhere to proper maintenance and quality assurance procedures for the airplane's horizontal stabilizer deice boots that led to the sudden in-flight loss of the partially secured left horizontal stabilizer leading edge and the immediate severe nose-down pitch-over and breakup of the airplane. The NTSB also determined that contributing to the cause of the accident was the failure of the Continental Express management to ensure compliance with the approved maintenance procedures, and the failure of FAA surveillance to detect and verify compliance with approved procedures.
On September 11, 1991, about 1003 Central Daylight Time, Continental Express Flight 2574, an Embraer EMB-120 operating under Title 14 of the Code of Federal Regulations, Part 135, experienced a structural breakup in flight and crashed in a cornfield near Eagle Lake, Texas. The two flight crewmembers, one cabin crewmember and 11 passengers aboard the airplane were fatally injured.

The NTSB analysis led to the following synopsis of the accident sequence:
- The airplane was descending at 260 KIAS. As the airplane descended through 11,500 feet, the leading edge of the left horizontal stabilizer separated from the airframe. The loss of the leading edge exposed the front spar of the left side of the horizontal stabilizer to the airstream, and an aerodynamic stall occurred that greatly reduced the down force produced by the horizontal stabilizer. The reduction in down force created a large nose-down pitching moment, and the airplane pitched down immediately.
- The airframe remained intact (minus the leading edge) for approximately 6 ½ seconds. The airplane's altitude was 9,500 feet, and it was flying at an airspeed of 280 KIAS when the left wing failed, and the right-wing tip detached from the airplane.
- The airplane then rolled to the right as the aircraft picked up speed toward the ground. The horizontal stabilizer and left engine separated from the airframe. The airplane then entered a spin to the right and fell uncontrollably toward impact.
The examination of the wreckage confirmed that the airplane had experienced an in-flight fire that occurred after, not before, the in-flight breakup. The failure of the left wing released fuel that probably led to the in-flight fire.

The horizontal stabilizer, or top of the T-type tail, had separated from the airplane before impact and was lying about 650 feet west-southwest of the main wreckage. Some of the structure and skin from approximately the upper third of the vertical stabilizer were still attached to the horizontal stabilizer. The lower two thirds of the vertical stabilizer remained attached to the tail cone in the main wreckage. The leading edge/deice boot assembly for the left side was missing from the horizontal stabilizer. The left side leading edge/deice boot was later found by investigators about 3/4 mile west of the main impact site.
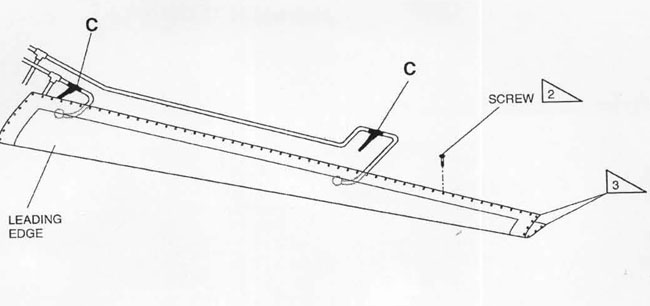
During the safety board's examination of the wreckage, none of the 47 screws that would have attached the upper surface of the leading-edge assembly for the left side of the horizontal stabilizer was found. There was no evidence of distress in the upper attachment holes for the left side leading edge assembly or indication that the attaching screws were installed when the left side leading edge assembly separated from the horizontal stabilizer. In addition, a "lip" was formed on the forward-most frame on the left lower side of the horizontal stabilizer spar cap. That frame (spar cap), with receptor holes for the lower attaching screws, was the area into which the screws mounted the underside of the left side leading edge assembly to the stabilizer. This lower frame area showed signs of distress.

The lower attachment screws remained installed, but the leading-edge assembly had separated from the stabilizer, with the exception of a small portion of composite structure remaining below the two farthest inboard screw heads. The spar cap on the lower left side of the horizontal stabilizer showed evidence of being pulled down so that it would project into the wind stream along with the leading edge. This pulling damage is consistent with the left side leading edge assembly having been ripped down and away from the lower attaching screws as it separated from the horizontal stabilizer. This evidence was consistent with screws missing on the top side of the left leading-edge assembly, and the lower attaching screws holding fast, pulling down the frame (spar cap) on the lower side of the stabilizer, and thereby forming the lip.


Photo of the upper attachment (no screws) - Photo of the lower attachment (with screws)
Horizontal Stabilizer Maintenance
On September 10, 1991, the night before the accident, Continental Express' Maintenance Control office scheduled horizontal stabilizer leading edge deice boots on N33701 for replacement. The airplane was pulled into the Continental Express hangar at Houston Intercontinental Airport (IAH) during the second shift at about 2130 hours for scheduled maintenance. The scheduled maintenance included the removal and replacement of both left and right horizontal stabilizer deice boots.

Photo Copyright Antonio Saraiva - used with permission
A change of either the left or right deice boot required that the leading edge/deice boot assembly for that side of the horizontal stabilizer be removed from the stabilizer. Normally, while still attached to the stabilizer, the old deice boot would be stripped from the composite structure of the leading edge, the deice lines would be disconnected, and the leading edge would be removed and a new deice boot bonded on. Then, the leading edge/deice boot assembly would be reinstalled on the horizontal stabilizer by means of approximately 47 attaching screws for each of the top and bottom sides of the assembly.

View Larger
{kind=link}
Two second shift mechanics, with the assistance of an inspector, gained access to the T-tail, which was about 20 feet above the ground, by means of a hydraulic lift work platform. The work was assigned by the second shift supervisor who took charge of N33701. The two mechanics removed most of the screws on the bottom side of the right leading edge and partially removed the deice boot bonded to the front of the right-side leading edge.
View Continental Express EMB-120 In-flight Structural Breakup Animation below:
The inspector who had climbed on top of the T-tail had removed the attaching screws on the top of the right side leading edge and then walked across the T-tail and removed the attaching screws from the top of the left side leading edge. The bottom screws that continued holding the horizontal stabilizer leading edge assembly in place were not removed. The top sets of attaching screws for both the left and right horizontal stabilizer leading edge assemblies were not visible from the ground.
Photo Copyright Antonio Saraiva - used with permission
The right leading-edge assembly was removed from the horizontal stabilizer following a shift change by third shift mechanics and a new deice boot was bonded to the front of the leading edge. During the third shift, the accident airplane was pushed out of the hanger to make room for work on another airplane. There was no direct light placed on the airplane as it sat outside the hangar. Work on the horizontal stabilizer was resumed outside where the third shift mechanics reinstalled the right-side leading-edge assembly.
The second shift work on the accident airplane was indicated on the second shift inspector's written turnover sheet; however, the incoming third shift inspector reviewed the sheet before the entry was made. The third shift maintenance supervisor and mechanics were not verbally informed of the removal of the upper screws on the left side leading edge. The maintenance work cards had originally been assigned to the third shift for completion, but the second shift supervisor elected to start work on the deice boots to assist the third shift with the workload. In addition, he did not issue the work cards to the second shift mechanics because they were in a package assigned to the third shift. As a result, no entries were made on the work cards that would have informed the third shift supervisor and third shift mechanics that work had been started by the second shift on both the left and right horizontal stabilizer deice boots.
A third shift inspector reported that he had gained access to the top of the horizontal stabilizer to assist with the installation and inspection of the deice lines on the right side of the horizontal stabilizer. He stated that he was not aware of the removal of the screws from the top of the left leading-edge assembly of the horizontal stabilizer. In the dark outside the hangar, he did not see that the screws were missing from the top of the left side leading edge assembly for the horizontal stabilizer.

Photo Copyright Kyle Donagher - used with permission
Systemic Issues
A major concern in this case was whether the problems noted represented aberrations related to individual maintenance personnel (there were several) or rather reflected systemic issues related to company policy. The influence of senior managers is often less tangible than that of line employees. However, the effects of management policy can be profound, and pervasive, affecting the company at all levels. For accident prevention purposes, it is important to determine at what level of the company structure--from the hangar floor to the highest executive--that attention should be focused to correct the problems that were discovered in this investigation.
The NTSB in their investigation concluded that the maintenance issues were not related solely to the actions of individual employees who were in the hangar the night before the accident. In fact, mechanics, supervisors, and inspectors from two shifts failed to follow proper turnover processes and were in noncompliance with General Maintenance Manual (GMM) procedures. Another problem noted was the definition of work on the horizontal stabilizer leading edge not having been identified as a "required inspection item" (RII). These items suggest a general disregard for following established procedures on the part of maintenance department personnel.
In this accident, the NTSB was confronted with a situation in which established company procedures were not being followed by personnel in the hangar. Inspectors, who were responsible for assuring the quality of work in accordance with established procedures, were among the worst offenders. The NTSB concluded that if Continental Express had had an effective quality assurance program, the company would have detected the procedural deficiencies noted during this investigation. The investigation revealed that the maintenance department personnel were generally aware of the correct procedures. Consequently, the lax attitude of personnel in the hangar suggests that management did not establish an effective safety orientation for its employees.
NTSB Board Member, Dr. John K. Lauber, went even further in his dissenting statement as part of the NTSB's report stating that he was "... perplexed by the majority decision that the actions of Continental Express senior management were not causal in this accident" and that the number of errors made by numerous individuals "... is not consistent with the notion that the accident resulted from isolated, as opposed to systemic, factors."
Dr. Lauber also stated that "By permitting, whether implicitly or explicitly, such deviations to occur on a continuing basis, senior management created a work environment in which a string of failures, such as occurred the night before the accident, became probable. Accordingly, their role must be considered causal in this accident." The complete text of Dr. Lauber's dissenting statement can be found beginning on page 52 of the NTSB Accident Report, which is linked in the Accident Board Findings section of this module.
Fifteen months following this accident, on December 9, 1992, another Continental Express EMB-120 was involved in an incident investigated by the NTSB. In this incident, shortly after takeoff the first officer felt a vibration through the airframe and the control column. The captain felt the same vibration and elected to execute a precautionary landing at the departure airport. The investigation revealed that 14 screws were missing from the left upper aileron vane and that the screws had been left out after the vane was partially removed during maintenance prior to the flight. The assigned mechanic did not replace the screws and the quality control inspector failed to see that they were missing during his inspection. (Reference: NTSB Incident Report FTW93IA048)
The NTSB determined that the probable cause of this accident was the failure of Continental Express maintenance and inspection personnel to adhere to proper maintenance and quality assurance procedures for the airplane's horizontal stabilizer deice boots that led to the sudden in-flight loss of the partially secured left horizontal stabilizer leading edge and the immediate severe nose-down pitch-over and breakup of the airplane. Contributing to the cause of the accident was the failure of the Continental Express management to ensure compliance with the approved maintenance procedures, and the failure of FAA surveillance to detect and verify compliance with approved procedures.
The NTSB issued 19 findings regarding this accident. The findings dealt variously with the:
- Lack of compliance with the General Maintenance Manual (GMM) procedures by the Continental Express maintenance department
- Improper quality control of work performed on a critical aerodynamic surface
- Improper classification of required inspection items (RII)
- Failure of airline management to instill an adequate safety orientation in its maintenance personnel by emphasizing the importance of adhering to procedures, and
- Inadequate surveillance of the Continental Express maintenance department by the FAA
Select this link to view the detailed NTSB Findings
Select this link to view the entire NTSB Report
The NTSB issued four recommendations. The subject areas covered include:
- Conduct a review of the regulations, policies, and practices related to required inspection items (RII)
- Study the feasibility of developing a means to advise flight crews about recent maintenance actions taken on their airplane
- Enhance flight standards surveillance of Continental Express
- Enhance flight standards Program Guidelines, including the National Aviation Safety Inspection Program, to emphasize hands-on inspection of equipment and procedures, unannounced spot inspections, and the observation of quality assurance and internal audit functions.
The complete text of the recommendations, excerpted from the NTSB report, is available at this link: NTSB Recommendations
In September 2000 the FAA released Advisory Circular (AC) 120-72, Maintenance Resource Management Training. Maintenance Resource Management (MRM) training is an aircraft maintenance variant on the more widely known Crew Resource Management (CRM) training. The AC presents guidelines for developing, implementing, reinforcing, and assessing MRM training programs for improving communication, effectiveness, and safety in maintenance operations.
MRM is a team-based safety behavior. It teaches managers and maintenance personnel skills that enable them to work safely in a complex system. MRM teaches more than just team skills; it teaches and reinforces an organizational philosophy in which all members of the organization are oriented toward error-free performance.
Like CRM, MRM training emphasizes a team approach to human error reduction using principles that seek to improve communications, situational awareness, problem solving, decision making, and teamwork. Unlike traditional coercive and hierarchical top-down safety programs, MRM advocates a decentralized, human-centric approach to safety. MRM encourages work teams to communicate vital operational risk and safety information directly and informally, regardless of rank or position, thus permitting rapid response to prevent impending crises.
The following key safety issues were identified from this accident:
- The operator had an inadequate inspection and maintenance program
- The failure of the operator's senior management to establish a corporate culture which encouraged and enforced adherence to approved maintenance and quality assurance procedures
- FAA surveillance of the operator was inadequate because it failed to identify and correct deficient management actions and oversight of the operator's maintenance department, as well as to identify practices in the maintenance program that were contrary to the approved maintenance manual
There are many examples of deficiencies in following specified maintenance tasks, and/or incomplete maintenance. Two representative examples of maintenance lapses that serve as precursor events are as follows:
- February 1987, BAe 146, Pacific Southwest Airlines. Following an uncontained engine failure, it was discovered that engine oil was contaminated with metal chips, and the engine oil filters had been operating in bypass mode for at least 40 days. With the exception of changing the oil and filter three times in the three months prior to the incident, no maintenance action had been taken to correct the root cause, which was generation of metal chips by the engine as it experienced a progressive internal failure. The NTSB determined that the contaminated oil contributed to the failure of the number four turbine bearing, leading to the uncontained failure of turbine blades.
- June 1990, Douglas DC-9-31, Eastern Airlines. During takeoff, a tire failure caused tire debris to be ingested in an engine, leading to an engine failure and subsequent return and engine-out landing. NTSB investigation revealed that the failed tire had been recapped 7 days prior to the incident and installed on the airplane two days prior to the incident. The NTSB concluded that the tire had been underinflated, and while undergoing maintenance checks on the day of the incident, tire pressure had not been checked with a gauge, allowing the underinflation to go undiscovered. Several other tire-blowout events on other airplanes had been related to tire underinflation.
Airplane Life Cycle:
-
Maintenance / Repair / Alteration
Accident Threat Categories:
- Structural Failure
- In-flight Upsets
Groupings:
-
Loss of Control
Accident Common Themes:
- Organizational Lapses
- Human Error
- Pre-existing Failures
Organizational Lapses
The approved procedures in the GMM were not followed by the maintenance, supervisory, and quality control personnel directly charged with evaluating the airworthiness of the aircraft before it was returned to service. Furthermore, NTSB investigators discovered two previous maintenance actions taken on the accident aircraft, each of which departed from the approved procedures. A detailed examination of the organizational aspects of the maintenance activities the night before the accident reveals a pattern of crossed lines of supervision, communications, and control. There was a failure of management to ensure compliance with air carrier policy and a failure to establish an effective safety orientation for its employees.
Human Error
Errors were made by numerous individuals. The most important of these was the proper hand-off procedures from the second shift personnel to the third shift personnel.
- The second shift supervisor failed to solicit a verbal shift turnover from the two mechanics he had assigned to remove the deice boots, failed to pass that information to the third shift supervisor, failed to complete the maintenance shift turnover form, and failed to ensure that the mechanics who had worked on the deice boots had filled out the work cards so that the third shift supervisor could review them.
- The second shift inspector failed to give a verbal shift turnover to the oncoming third shift inspector.
- The second shift mechanic failed to give a verbal shift turnover to the second shift supervisor or to the oncoming third shift supervisor and failed to solicit the work cards from the second shift supervisor.
These errors suggest a lack of attention to established requirements for performing maintenance and quality control in accordance with the GMM.
Preexisting Failures
The upper row of fasteners for the left horizontal stabilizer leading edge had been removed during scheduled maintenance the night before the accident, and a breakdown in procedures failed to detect that the work was incomplete. The subsequent separation of the leading edge of the horizontal stabilizer on the accident flight led to an aerodynamic condition from which the flight crew could not recover.
There are many examples of airplane accidents where important tasks have been improperly accomplished due to safety gaps in the "handoff" from one person/organization to another. Two examples of these deficiencies are illustrated by these two accidents:
Eastern Airlines Flight 401, December 1972, Lockheed L-1011. On approach to Miami, the flight crew focused on an apparent unlock indication of the nose landing gear (the gear did not indicate that it was down and locked) and did not assign duties such that one crew member continued to fly the airplane and monitor flight critical information. The autopilot, which had been engaged while the crew accomplished various troubleshooting procedures, inadvertently disconnected, and was not noticed by the crew. The airplane began a gradual, unmonitored descent, and crashed into the Everglades. The first officer had asked the captain who should fly the airplane and got no response and did not repeat the question. He did not assume flying duties, and the flying duties were not formally handed off, or traded, between the captain and first officer.
See accident module
Air Florida Flight 90, January 1982, Boeing 737-200. During a takeoff attempt from Washington National Airport, the airplane crashed into the Potomac River. It was later determined that the airplane's wings were contaminated with ice, and further, that engine sensors, critical to proper power setting, were plugged by ice. The combination of a low thrust setting and wing contamination led to the crash. The airplane had been deiced prior to takeoff. The deicing was performed under contract by another airline's maintenance department. Following deicing of the left side of the airplane, deicing was interrupted, and completed later by another deicing crew, using different procedures, and a different deicing fluid mixture. Although it could not be concluded by the investigators that the inconsistencies involving the deicing procedures contributed to the accident, it was revealed that the procedures used on both the left and right side of the airplane were not consistent with deicing operations required by Air Florida.
See accident module
Technical Related Lesson:
Certain maintenance tasks, if not completed properly, can have an immediate and severe adverse impact on flight safety. (Threat Category: In-flight Upsets)
- The loss of the leading edge of the horizontal stabilizer caused an irrecoverable aerodynamic upset. The maintenance procedures involved in this accident were focused on the removal and replacement of the deice boots, not taking into account that this required the removal of an aerodynamic surface (horizontal stabilizer leading edge), the loss of which would cause an uncontrollable in-flight upset. While nearly all maintenance activities have safety implications, the loss of an aerodynamic surface, as occurred in this accident, resulted in immediate loss of control, and catastrophic consequences.
Common Theme Related Lessons:
Safety tasks that are initiated by one person/group but will be completed by another person/group present an especially important communication challenge. Robust processes must be in place to ensure that these tasks are correctly and consistently completed. (Common Theme: Organizational Lapses)
- The Continental Express General Maintenance Manual (GMM) had FAA-approved procedures for shift turnovers. These procedures included briefings by mechanics to supervisors, briefings by outgoing supervisors to incoming supervisors, completion of maintenance and inspection shift turnover forms (so that oncoming personnel would be aware of incomplete work), and the documentation of incomplete work that would be noted by the mechanic on the reverse sides of work cards. These procedures were not followed. The NTSB concluded that the GMM contained clear procedures, which, if followed, could have prevented the accident.
A management emphasis on safety is needed to ensure that safety permeates the entire organization. (Common Theme: Organizational Lapses)
- The NTSB concluded that Continental Express management had failed to establish a corporate "safety culture" which would encourage and enforce adherence to approved maintenance and quality assurance procedures. It was further concluded by the investigators that this led to a general disregard for established procedures.