
Airbus AS350B2
Liberty Helicopters, Inc., N350LH
Flushing, NY
March 11, 2018

On March 11, 2018, at approximately 1908 hours local daylight time, an Airbus model AS350B2 helicopter performed an autorotative descent and ditching on the East River in New York City following an inadvertent engine shutdown due to fuel starvation. The flight was conducted under 14 CFR Part 91 as an aerial photography flight with the helicopter doors removed or secured in the open position. The helicopter capsized shortly after landing in the water due to insufficient and asymmetrical flotation system inflation. Because of a harness and tether system securing the passengers to their seats, they were unable to extricate themselves prior to the helicopter becoming submerged in the water. The single pilot survived with minor injuries, the five passengers onboard drowned, and the helicopter was substantially damaged.
The NTSB concluded that the front passenger’s tether had inadvertently activated the helicopter’s fuel shut off lever (FSOL) while the passenger was in motion and maneuvering in his seat. The lack of a quick-release harness system contributed to the passengers being unable to free themselves and egress the helicopter in a timely manner. Additionally, the incomplete activation of the rigging and improper inflation of the flotation equipment resulted in the helicopter capsizing and rolling inverted in the water, likely leading to the passengers being unable to exit the aircraft.
NTSB accident report: ERA18MA099
History of the Flight

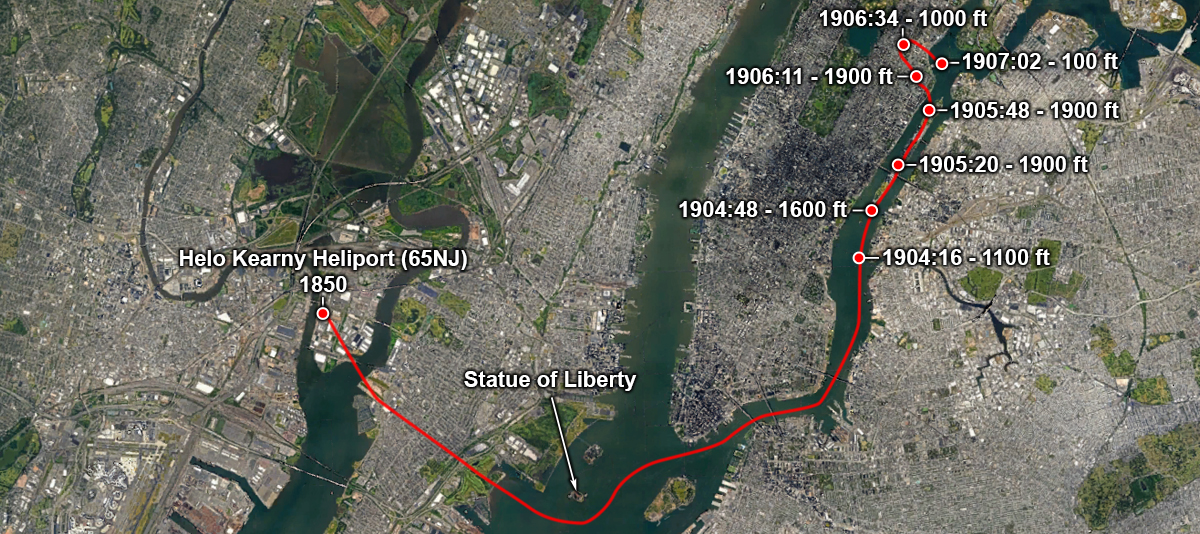
The 14 CFR Part 91 Visual Flight Rules (VFR) flight departed from Helo Kearny Heliport (65NJ) on March 11, 2018, about 1850 eastern daylight time. This was planned to be a 30-minute local flight and no flight plan was required nor filed. The flight proceeded south towards the Statue of Liberty at or below 500 feet above ground level (AGL). After passengers photographed various landmarks, the flight proceeded east, then the pilot requested a clearance to go north up the East River. The controller cleared the flight to proceed along the route to the north end of Central Park at or below 2,000 feet mean sea level (MSL). At 1905:44, the flight had climbed to 1,900 feet and turned northwest over Manhattan towards Central Park. At approximately 1906 the engine lost power. During the autorotative descent, the pilot activated the inflation of the floats. The helicopter descended to the East River where it became inverted due to asymmetric float inflation. The pilot was able to extricate himself from the helicopter; however, the five passengers were unable to release their harnesses and drowned.
Purpose of Flight
The flight was marketed as an aerial photography flight by NYONair and operated by Liberty Helicopters under contract. The flight was flown with the doors secured in an open position or removed. This allowed passengers to extend their feet and legs outside the helicopter while taking photographs. The flight was a customizable operation, as passengers could provide route input based on which landmarks they wanted to photograph.
Accident Sequence
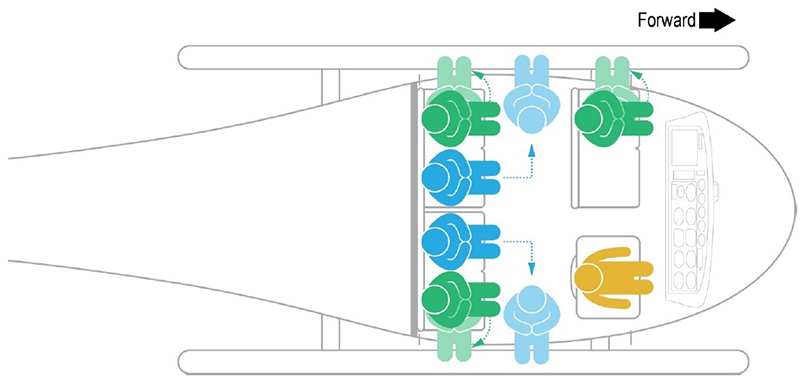
The accident helicopter contained an onboard video camera mounted in the cabin that recorded the accident sequence. The camera’s field of view included the left front passenger but did not include the area of the floor between this passenger and the pilot. It is common for tour/sightseeing helicopters to carry a passenger in the left front seat.
This AS350B2 helicopter incorporates three control levers mounted on the floor between the two front seats. Normally the flight controls (cyclic, collective) are removed from the passenger side of the cockpit for tour operations, but other controls may be nearby the passengers. For this model of helicopter, the three levers are for the rotor brake, the fuel shutoff lever (FSOL), and fuel flow control lever (FFCL). The FSOL has a small piece of safety wire to hold it in position so the pilot cannot inadvertently move it. However, the wire can be easily broken when the pilot needs to intentionally move the lever, such as shutting off the fuel supply in a ditching. The FFCL has detents to prevent the pilot from inadvertently moving it out of position.
Digital recordings showed that at around 1905 the front passenger was facing to the left to take photographs and leaning back to get his feet in camera range. As the passenger maneuvered in the seat, the loose tether on the back of his harness dangled near the floor-mounted controls between the front passenger seat and the pilot seat. Around 1906, the passenger appeared to sit more upright, but the tether was pulled taut and then "popped" upward as if it had loosened. Approximately two seconds later, ambient engine noise could be heard decreasing in the audio from the mounted camera. The helicopter started to descend. The pilot realized the loss of engine power and began procedures for an autorotative descent, troubleshooting, and landing decision.
The helicopter was equipped with inflatable floats, so the pilot decided a landing in the river was safer than attempting a landing in Central Park, which included trees, pedestrians, and other obstacles. The pilot turned east toward the East River and attempted an engine restart, which was unsuccessful. Once committed to the water landing, in accordance with emergency procedures, he reached for the FSOL to shut off the fuel, but realized it was already in the up (cutoff) position. He noted the front passenger’s tether in the vicinity of the floor-mounted controls. The pilot then moved the lever back to the down position to restart the engines, however there was not enough time to attempt another engine restart.
At approximately 1907, the pilot activated the inflatable flotation system. An audible "pop," increased drag, and visual indication of the floats inflating confirmed the floats had deployed. The helicopter touched down on the water about 20 seconds later.
While the helicopter landed upright in the water, it began an immediate roll to the right and was completely submerged and inverted within 11 seconds of touchdown. The pilot tried to release the front passenger’s tether for escape but was unable. The helicopter was submerged before the pilot released his own restraint and was able to egress. A tugboat quickly arrived and rescued the pilot. Emergency response resources had divers in the water to recover the passengers by 1925; however, none of the passengers were able to egress on their own and did not survive. The helicopter did not sink and was later secured to a pier, still inverted. It was noted that the three floats on the right appeared less inflated than those on the left.
Part 91 Versus Part 119/135/136
Normally this type of flight would be considered a commercial air tour and would have been conducted under 14 CFR Part 91 and Part 136 of the flight rules. While Part 91 applies to any aircraft in flight, the Part 119, 135, and 136 rules add additional requirements when carrying passengers for the purpose of air commerce and common carriage. There are many nuances in the rules for commercial air tours since they can be conducted in a variety of aircraft and locations.
To simplify the rules, Part 119 describes requirements to get an air operator certificate. Part 136 describes the safety standards for air tours, as well as the definition of an air tour. However, under 14 CFR 119.1(e), there are some exceptions to the applicability of this part. One of these exceptions is 14 CFR 119.1(e)(4)(iii), which is "aerial work operations" and includes "aerial photography or survey." NYONair was using this exception to fly their flights under Part 91 and being excepted from Part 136.
The original intent of the Part 119.1(e)(4)(iii) rule was to allow for professional photography, such as news reporting, site surveys, and film and publication production. It was not intended for tourism purposes. However, the FAA did not define "aerial photography," so NYONair was legally operating under all applicable Part 91 rules. Part 136 was also applicable to the operation and Liberty met all Part 136 rules. Liberty Helicopters, as a contractor to NYONair, is a certified Part 135 operator, and for air tours would normally operate under the 135 certificate in addition to the Part 119 and Part 136 rules required for air tours. NYONair and Liberty Helicopters held the necessary paperwork and Letters of Authorization (LOA) to operate as an aerial photography provider.
The table shows the relationship between the operating rules. Also reference Appendix B in the NTSB accident report which highlights more details in required oversight areas.
| Title of operational regulation | Part # | What it does for commercial operations |
|---|---|---|
| General Operating and Flight Rules | 91 | Basic requirements for aviation operations in U.S. airspace. |
| Certification: Air Carriers and Commercial Operators | 119 | Provides a framework for applicability of requirements for commercial operations and air carriers. |
| Operating Requirements: Commuter and On-Demand Operations and Rules Governing Persons on Board Such Aircraft | 135 | Additional requirements for passenger-carrying operations. More stringent FAA oversight. Liberty qualified for these operations when not under contract to NYONAir/FlyNYON. |
| Commercial Air Tours and National Parks Air Tour Management | 136 | Additional, specific requirements for commercial air tours and national park air tours. |
An agreement also existed between the NYC Economic Development Council and the Helicopter Tourism and Jobs Council to reduce noise in the vicinity of JRB Heliport in Manhattan by eliminating tours on Sundays. Liberty flew most of their own Part 135 air tour flights from this heliport. The accident report states that due to this loss of revenue, Liberty agreed to accept NYONair as a customer because they would fly out of New Jersey, and the Part 91 flights were "aerial photography" flights and were not restricted by the noise agreement.
Passenger Restraint Systems
Primary and supplemental restraints were both used during the flight. These restraints, along with a safety briefing, were discussed prior to flight and are described as follows:

Primary restraint – Each seat was equipped with a Part 27 type-certified, FAA-approved restraint system (seat belts) that were required to be used for takeoff and landing. Once the pilot allowed the passengers to remove the FAA restraint system, they could maneuver in the cabin to take photographs and the supplemental restraint system would prevent them from falling out of the helicopter.
Supplemental restraint – Due to the safety issues of unstrapping from the FAA-approved seat restraints to maneuver within the helicopter and allow passengers to place their feet out a side door, the operator provided an Occupational Safety and Health Administration (OSHA)-approved safety harness that NYONair required all passengers to wear. A long leash, or tether, was attached to a D-ring on the back of the harness, and the restraints are then tethered to the floor of the helicopter using a locking carabiner. This is a carry-on system that is not permanently installed. It is not subject to Part 21 (products and parts) design approval nor is it considered a major alteration (Form 337).
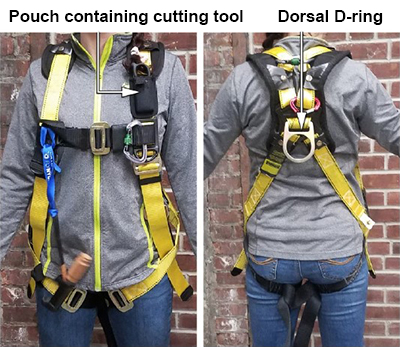
Harness description – The harness/tether system was not part of the rotorcraft type design, nor required for flight. The harness system was suggested and developed by NYONair company personnel and others in the film industry. It consisted of an off-the-shelf, fall-protection workplace harness that is yellow and referred to as the "yellow harness." The passengers are secured to the helicopter floor through use of a tether that is attached to a D-ring on the back of the harness and to the helicopter floor with a screw-type locking carabiner at both ends of the tether. The passengers could not reach their own carabiner on the harness or the floor. The length of the tether varied depending on where the passenger was seated. This allowed passengers in the middle seats to access the doorway.
Alternate harness – There was a second type of harness available for use. These were blue in color and referred to as the "blue harness." These were made by Air Rescue Systems and met the FAA's Technical Standard Order, TSO-C167, for human harnesses. The blue harness had multiple attach points for the carabiner, and it was possible for the passenger to reach their own carabiner depending on where it was attached. The company generally used these harnesses for smaller passengers and only had a few of them on hand. None of the blue harnesses were used on the accident flight.

Cutting tool – The passengers were also provided with a tethered cutting tool to cut the harness in the event of an emergency. The tools were of two different models, each marketed as seat belt or safety cutters.
Safety briefing – During the pre-flight briefing and prior to boarding, the passengers watched a safety video regarding donning and removing the harness and untethering themselves or each other by opening the carabiner. In the event the locking carabiner could not be reached or opened by hand, each harness had a cutting tool that the passenger could use to cut the harness or tether in the event of an emergency. However, neither the safety briefing video nor the employees attaching the harnesses to the passengers explained how and where to cut the harness or tether. An employee was required per the company training manual to ask the passengers for questions about the video. For this accident flight, there were no questions asked. The harnesses were OSHA-approved for fall protection, but were not designed to be quick release and did not require FAA approval for use on these flights.
Helicopter Flotation System
The accident helicopter was equipped with an emergency flotation system manufactured by Apical Industries (Dart Aerospace). It was installed through use of a Supplemental Type Certificate (STC) on the helicopter. The system consists of six individual floats, three per side, that inflate when activated by the pilot. The activation lever is mounted on the cyclic and designed to be single-handedly triggered by the pilot. The lever is similar in look and operation to the brake lever mounted on a bicycle handlebar and is actuated the same way by keeping a hand on the cyclic and reaching for the lever with fingers. A small shear pin locks the handle in place to prevent inadvertent activation and is designed to break with a pull force of 12 pounds. The lever is connected by a small cable that is routed to a junction box which then branches out to two cables. Each cable goes to a reservoir (bottle) of compressed nitrogen which discharges into either side of the floats. If one of the bottles does not discharge, there is a crossover hose between the left and right floats to inflate both sides equally, although they would be less than fully inflated.

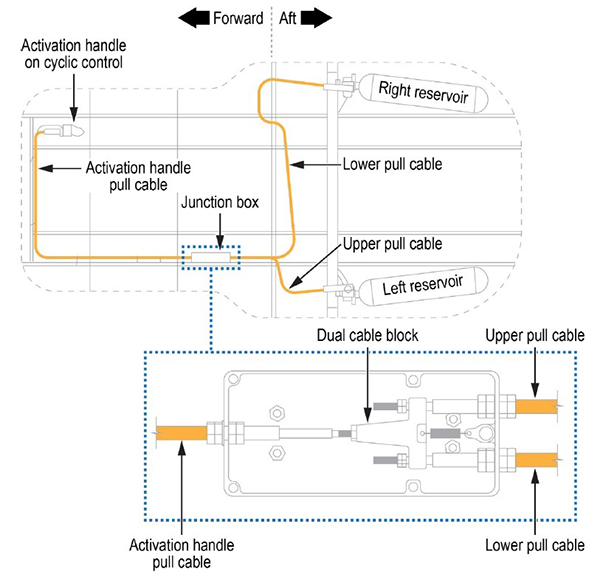
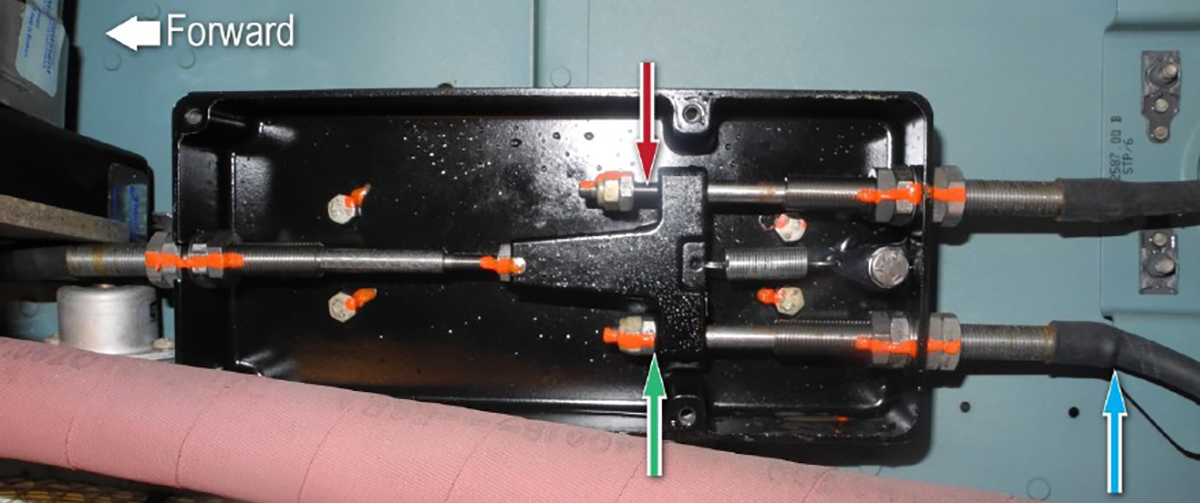
It was determined by investigators that only one nitrogen bottle had discharged during the pilot activation of the system. There is also evidence that only one of the cables exiting the junction box pulled far enough to activate the one bottle (red arrow), and the other cable appears to not have moved enough (green arrow). That same cable also has a greater bend (smaller radius) after exiting the junction block (blue arrow). The pilot stated that the activation lever was hard to pull, and that he used his left hand to hold the cyclic and used his right hand to pull the lever as far as he could until he heard a bang noise and visually saw the floats begin to inflate.
Even if the flotation system is not used, it must be tested/activated every 36 months per the STC. This is usually done in a hangar with the pilots performing the activation. It was known by Liberty pilots that high forces were required to activate the system and they all used the technique of holding the cyclic with their left hand while activating the system with their right. Investigators questioned other operators using the same float system. One operator in Alaska said they could easily pull the lever with two fingers, while a Canadian operator had similar results as Liberty and said it was “common knowledge” among its pilots that high pull forces and two hands were needed for the operation. In many tests it was not unusual for only one bottle to discharge after pilots heard the bang. In the case of the accident helicopter, the pilot stated that after pulling the handle as far as possible, hearing a bang, and seeing both left and right floats inflating, he assumed the system was operating correctly.
During post-accident testing in a pool of water with a weighted test rig, investigators discovered that even if one bottle had fired and equally inflated all floats, there was still not enough inflation for the helicopter to remain stable in the water.
The flotation system was certified for use on the helicopter through an STC approved by the FAA in 1997. After this accident and subsequent testing, the FAA accepted a maximum pull force for the handle as proposed by the STC holder. The Rotorcraft Flight Manual Supplement and the Maintenance Manual Supplement for the system have since been updated with this information. Investigators determined that the required pull forces, as well as a specific technique to pull the activation handle, are not specified in the original design requirements or STC documents. This led to ambiguity among pilots and operators over whether the system was working correctly and the "common knowledge" techniques and cues as to whether the system has activated properly.
| Title of design and manufacturing regulation | Part # | Specifics of design and manufacturing requirements |
|---|---|---|
| Certification Procedures for Products and Articles | 21 | Process requirements for certification of aircraft design and manufacturing. STC for flotation device is issued under this part. |
| Airworthiness Standards: Normal Category Rotorcraft | 27 | Flotation devices must be compatible with and maintain these standards (e.g., controllability, performance, gross weight, etc.). |
Investigators were concerned that other flotation systems installed via STC may also have the same issue. They were also concerned that the rotorcraft Advisory Circulars (AC 27 and AC 29) do not provide any guidance on human factors issues related to activation or deployment of flotation systems. The NTSB recommended that the FAA revise these ACs to include design objectives "such as activation handle pull-force characteristics; provisions for clear, unambiguous, and positive feedback to pilots to indicate that the float system was successfully deployed; and inspections to ensure that an installation of a manual activation system does not preclude a pilot's ability to deploy the floats, as designed, after it has been fielded."
Conclusion
Investigators determined this accident could have been survivable. The inadvertent engine shutdown event and subsequent water landing were handled correctly by the pilot. Unfortunately, other issues intervened in a complex, but predictable manner. For safety purposes, the passengers were secured to the helicopter for operation with the doors open, but were subsequently unable to untether themselves and quickly egress in an emergency.
There was need for a deployable flotation system which did not activate correctly in this accident. Malfunctions in the design resulted in an insufficient and asymmetric inflation of the floats that could not keep the helicopter upright.
Additionally, the operation was being conducted under a section of regulations which allowed for less FAA oversight and requirements based on an ambiguous definition of the type of operation being flown. Issues associated with passenger interference with flight controls, passenger restraints, and the flotation system activation methods were known by NYONair and Liberty, and in some cases being addressed; however, the concerns were not resolved at the time of the accident.
The NTSB concluded that "Liberty and NYONair exploited the exception at 14 CFR 119.1(e)(4)(iii), allowing aerial photography flights to be operated under Part 91, thereby avoiding the additional FAA requirements and oversight that apply to commercial air tours conducted under either Part 135 or Part 91 with an air tour LOA."
The following NTSB findings are relevant to this module:
- The front passenger’s tether caught on the FSOL, resulting in fuel starvation to the engine and loss of engine power.
- The pilot successfully autorotated the helicopter and activated the float system on time; however, the floats did not inflate fully nor symmetrically, making the helicopter unstable in the water.
- Both Liberty's and NYONair's decision to use locking carabiners and ineffective cutting tools was inappropriate and unsafe.
- The landing was survivable; however, the provided harnesses did not allow a quick escape from the helicopter.
- The FAA's process for supplemental restraints does not provide guidance to inspectors to evaluate specific installations.
- Even though the flotation system crossover hose did not operate correctly, buoyancy testing showed that symmetrical inflation from only a single bottle discharge is still not enough to allow the helicopter to remain upright in the water.
- Flotation system pull-force limitations were not provided by Dart Aerospace. Therefore, a means to inspect and correct high pull forces cannot be performed.
- Although the pilot was aware that the flotation gas reservoirs may not inflate simultaneously, aural and visual cues and high pull forces on the activation handle led him to believe the floats would fully inflate.
A complete list of accident board findings can be found at: NTSB Findings
NTSB accident report: ERA18MA099
The NTSB issued the following urgent recommendation shortly after the accident:
NTSB Urgent Safety Recommendation ASR-18-12, (3/19/18) – Issued to the FAA and recommended prohibiting all open-door commercial passenger-carrying flights that use harness systems, unless the harness can be quickly and easily released.
The following is a summary of NTSB recommendations in the final report that are most applicable to this module:
- Modify supplemental restraint system approval process and inspector guidance (FAA)
- Revise CFR rules and definitions to bring all tour operators under similar standards (FAA)
- Review design, activation, and inspection of emergency flotation system (FAA)
- Modify floor-mounted FSOL (Airbus)
- Establish a Safety Management System (Liberty Helicopters and NYONair)
A complete list of recommendations can be found at: NTSB Recommendations
14 CFR 27.801 - Ditching – This is a general rule used if the rotorcraft is to be certified for ditching. The characteristics of the rotorcraft must be such that the probability of causing injury to occupants is minimized. This includes ensuring the rotorcraft will float and is buoyant, at least long enough to allow all occupants to egress to the required life rafts.
14 CFR 27.807 - Emergency exits – This rule describes the number, type, location, and operation of emergency exits for rotorcraft. Includes labeling and placard requirements.
14 CFR 27.1143(d) - Engine controls – This paragraph states that if there is a fuel shutoff feature, the control must have a means to prevent inadvertent movement of the control into the shutoff position.
14 CFR 27.1189(b) - Shutoff means – This rule is under rules for fire protection and states that the required fuel shutoff must guard against inadvertent operation, as well as allow the control to be re-opened if closed.
14 CFR 27.1415 - Ditching equipment – This rule mentions requirements for life preservers, rafts, and signaling equipment.
14 CFR 91.147 - Passenger – carrying flights for compensation or hire – This rule states general requirements and information required in a Letter of Authorization (LOA).
14 CFR 119.1(e)(4)(iii), and (e)(2) - General (under certification of air carriers and commercial operators) – These paragraphs state that Part 119 is not applicable to aerial photography or survey flights, or for tours in compliance with a LOA issued under 91.147.
14 CFR 135.183(d) - Performance requirements: Land aircraft operated over water – This rule simply states a helicopter flown over water must have flotation devices. The STC design satisfied this requirement.
14 CFR 136.9 - Life preservers for operations over water – This rule states when air tour operators need to provide life preservers to passengers.
14 CFR 136.11 - Rotorcraft floats for over water – This rule provides the requirements for when floats are needed.
STC SR00470LA - This is the STC for the flotation system installed on the accident helicopter. It was issued to Dart Aerospace for the installation of Apical Industries emergency flotation systems on multiple AS350 model helicopters. It was originally issued on November 17, 1997.
Technical Standard Order (TSO) TSO-C167 - Personnel Carrying Device Systems (PCDS) – Also known as human harnesses, this TSO describes the technical requirements. In this accident, human harnesses were not required, but the operators inventory consisted of both TSO and non-TSO models.
Advisory Circular (AC) 27-1B - Certification of Normal Category Rotorcraft – While this AC contains certification information on ditching and flotation systems, it does not consider human factors or any advice on pull forces or feedback on activation of deployable floats. The NTSB recommended to add content to address this issue.
During the investigation, it was determined that NYONair and Liberty had weak safety cultures and no formal safety management programs in place at the time of the accident. When the companies began working together, regular safety review meetings were attended by personnel from each company. While the NYONair CEO attended some early meetings, most of the meetings were run by pilots from both organizations. Liberty pilots reported that their safety concerns were never met with any action by NYONair. NYONair seemed to treat the concerns as suggestions and disliked using the term "issues." This eventually resulted in the Liberty pilots no longer being allowed to participate in the meetings.
While both Liberty and NYONair each had FAA-approved training manuals, these would not have been useful on the "FlyNYON" open door flights using Liberty’s helicopters. For example, Liberty pilots specifically raised concerns about the yellow harnesses and preferred the quick-release blue ones be used. NYONair stated the FAA only required the approved restraints (seat belts) for doors-off flights and believed that by using the yellow harnesses they were “going above and beyond” from a safety standpoint.
Liberty pilots also expressed concern on the effectiveness of the cutting tools, and even convinced NYONair to order some better tools, after the NYONair lead pilot had a hard time cutting through a piece of tether in a demonstration. However, the new equipment was not ordered in time for the accident flight.
Liberty pilots, including the accident pilot, were concerned with interference of the tethers with the floor-mounted controls and had moved tethers away from the controls on prior flights.
At one point, a disagreement between the NYONair CEO and a Liberty pilot (their safety officer) resulted in NYONair stating his services were no longer required on the doors-off flights.
- Ambiguity in regulations allowed the operator to avoid certain FAA oversight ‐ NYONair exploited the 14 CFR119.1(e)(4)(iii) rules for aerial photography, thereby avoiding additional FAA oversight that would normally apply to a commercial air tour.
- Inadequate passenger safety and equipment briefing ‐ The yellow harnesses used were not quick-release harnesses. The passengers were given one of two types of cutting tools but the safety briefing did not specifically show where to cut the harness or under what circumstances.
- Inadvertent activation of FSOL/critical aircraft controls ‐ The front seat passenger, while taking photos, caught his tether on and activated the FSOL, which shut off the fuel system.
- Inability of passengers to quickly release the restraint with minimal difficulty ‐ The carabiner clips that locked the harnessed passengers in the aircraft could not be easily reached or detached. The cutters for the harness were ineffective.
- Ineffective flotation system design and STC certification ‐ Although certified by the FAA with an STC, the flotation system did not work correctly. The system lacked documentation on pull forces to determine an effective installation. This could have revealed improper rigging and installation issues. Additionally, the flotation system was designed to provide adequate inflation of all floats with only one bottle discharged. In this accident, only one bottle discharged and resulted in asymmetrical and inadequate inflation. Post-accident testing showed that symmetrical inflation, with only one bottle, did not provide enough buoyancy and stability.
Critical controls are protected from inadvertent operation.
- Although the FSOL met regulatory requirements to protect against inadvertent movement, the front seat passenger's tether caught on the FSOL and actuated it, causing fuel starvation.
Passengers can easily release their restraints in the event of an emergency.
- NYONair provided additional restraints to prevent passengers from falling out of the helicopter. They did not adequately consider an emergency egress that allowed a quick release from the harness.
- The cutting tools were ineffective and insufficient for the passengers in this accident.
A certified flotation system will properly deploy.
- The flotation system is an FAA-certified STC kit; however, certain installation, operation, and maintenance guidance was not specified. The FAA oversight process failed to notice this shortcoming. Therefore, maintenance personnel did not have the direction or requirements needed to ensure the system would function as intended.
- The pilot assumed that the audible bang and visual cues of inflation indicated a proper deployment.
- Symmetrical inflation was not achieved, resulting in the aircraft capsizing.
Bell 206L-1, Commercial Helicopters, N5013F, West Delta 105, Gulf of Mexico, September 26, 1984
A Bell 206 performed an autorotative water landing off the coast of Louisiana after a total engine power loss. The right float was not fully inflated upon landing and the helicopter rolled right and became inverted. The sole occupant, the pilot, was not injured. The NTSB report cited pressure in the float assembly as too low.
NTSB accident report: FTW84LA414

Aerospatiale (Airbus Helicopters) AS350B, Turbowest Helicopters Limited, C-FHBG, High Prairie, Alberta, Canada, April 4, 1994
In 1994, a Canadian-registered AS350B crashed after a patient on a stretcher on the left side of the helicopter was adjusting a knapsack by his knee, which was located next to the FFCL. The FFCL was inadvertently pulled to the full up and aft position, which is the fuel cutoff/engine start flow position, resulting in fuel starvation of the engine. The helicopter experienced a hard landing.
TSB Canada accident report: A94W0037
Aerospatiale (Airbus Helicopters) AS350B1, Air Alpha Greenland A/S, OY-HEC, Ilulissat, Greenland, September 13, 1996
An AS350B1 was being used for aerial photography and filming of a movie. The photographer was seated in the left front seat and the helicopter with his equipment. The photographer experienced an equipment malfunction and moved about in his seat manipulating the equipment. He also turned and reached behind him where other equipment was stored. At this point the helicopter experienced a loss of power. The pilot initiated an autorotation and reached with his left hand to the FFCL, finding it "somewhere between open and closed." The pilot returned the lever to the open position but was unable to recover the aircraft before it impacted the water. It is the opinion of the investigation that "during his movements in and around the left-hand seat the photographer may unintentionally have pushed the fuel control lever out of the notch and up towards idle/shut down."
Danish AAIB accident report: HCL No 62/96

Sikorsky S-76C++, Petroleum Helicopters, N748P, Morgan City, Louisiana, January 4, 2009
A Sikorsky S-76C++ crashed after colliding with a red-tailed hawk which fractured the windshield and inadvertently moved the engine power levers to a low power/idle position. The crew was likely disoriented and unable to recover from the loss of power.
Library module: S-76 Petroleum Helicopters
Emergency Order of Prohibition, Docket No. FAA-2018-0243, 83 FR 12856 (03/26/18) ‐ "Doors-off and "Open-Door" Flight Prohibition: Emergency Restriction/Prohibition Order" – This emergency order prevents the use of any supplemental restraints that cannot be released quickly in an emergency in doors-off flight operations. It also prohibits doors-off flights unless the passenger is always secured using FAA-approved restraints.
Notice N 8900.456, 03/23/18 ‐ Emergency Order of Prohibition Pertaining to "Doors-Off" Flight Operations for Compensation or Hire – This is a Notice to Flight Standards inspectors on the process for issuing a letter of authorization for Supplemental Passenger Restraint Systems (SPRS) for operators. This was later revised in Notice N 8900.457, 04/10/18 and Notice N 8900.506, 04/10/19.
FAA Order 8900.4, 07/8/19 ‐ Emergency Order of Prohibition Pertaining to "Doors-Off" Flight Operations for Compensation or Hire – This order supersedes N 8900.506 and requires operators to cease using SPRS until flight standards personnel inspect restraints used by operators and issue an LOA for those restraints. The inspector must determine that the SPRS does not require the use of a knife to cut the restraint, the use of any other additional tool, or the assistance of any other person. An SPRS also must not require passenger training beyond what would be provided in a preflight briefing.
Information for Operators, InFO 18003 ‐ Supplemental Passenger Restraint Systems (SPRS) for “Doors-Off” Flight Operations Conducted for Compensation or Hire – This InFO recommends that Part 91 and Part 135 operators familiarize themselves with Order 8900.4.
Dart FMS-350(2) ‐ flight manual supplement
Dart Aerospace Service Bulletin SB-2018-03
Dart Aerospace Service Bulletin SB-2018-07 revision D (11/25/19) ‐ This service bulletin contains procedures for inspecting the pull cables on certain float kits, correcting any rigging issues, and contacting Dart, if needed.
Airbus Safety Information Notice 3951-S-00 ‐ This is a general notice to pilots of Airbus helicopters to be aware of, and mention in preflight briefings, the potential for passengers or their belongings to interfere with flight controls of critical system functions.
FAA SAIB AIR-21-13 (08/13/21) Engine Emergency Shutdown System ‐ This SAIB recommends owners and operators of AS350B2 and B3 helicopters modify the FSOL control per an Airbus Helicopters service bulletin to prevent the FSOL from accidentally being operated.
Airbus Helicopters Service Bulletin No. AS350-76.00.24 ‐ This service bulletin replaces the stop plate of the floor-mounted FSOL with a redesigned plate which forces the FSOL to be operated in two stages, so a single action will not activate it.
Safety Management Systems, docket number FAA-2021-0419 (05/28/24) ‐ Final rule to require certain certificate holders and air tour operators, including NYONair and Liberty, to develop and implement an SMS.
Notice of Proposed Rulemaking (NPRM), docket number FAA-2023-2250 ‐ This proposed rule would codify, with updates, the current Emergency Order of Prohibition regarding the use of supplemental restraints. This rule is effective Oct 21, 2024 and affects rules in Parts 1, 11, 91, 135, and 136.
When NYONair resumed doors-off flights without the harness/tether system, they required all passengers to always wear the FAA-approved restraints.
NYONair applied for, and received, a Letter of Authorization (LOA) with authorized doors-off flights which required them to use FAA-approved quick-release harnesses.
NYONair revised procedures for doors-off flights where passengers using a practice tether must demonstrate they can release from the restraint when given an egress command, as well as other improvements to the preflight video briefing.
Flotation system AD 2020-02-23, effective on February 28, 2020.
Emergency Equipment; Emergency Flotation Section AD 2024-20-07, effective on December 5, 2024.
Rotorcraft Life Cycle
- Operational
Accident Threats
- Fuel Related
- System / Component Failure or Malfunction (non-powerplant) (SCF–NP)
Industries
- Air Tour / Sightseeing
Accident Common Themes
- Organizational Lapses
- Flawed Assumptions
- Unintended Effects
Organizational Lapses
According to the investigation, it was concluded there were several issues with Liberty's management, NYONair's management, and problems with them working together.
Management control – Early in the partnership, Liberty management was closely engaged with NYONair management. However, as the number of flights increased, the daily supervision was delegated to Liberty's chief pilot. Eventually, the CEO of NYONair and their director of business operations managed the day-to-day operations while Liberty management became increasingly less involved. This resulted in NYONair having more influence in safety aspects of these Part 91 flights using the resources from Liberty. There were also personal conflicts between Liberty’s safety officer and the NYONair CEO.
Operational control – Liberty is a Part 135 operator, so its own flights were operated under its FAA-approved certificate and flight operations manual. However, the FlyNYON flights Liberty operated under contract were flown under Part 91 only. Since Liberty's Flight Operations Manual stated that they had operational control over the Part 91 FlyNYON flights, the company would fly them while maintaining the same level of safety responsibility as it did for their Part 135 Liberty flights. However, investigators realized that NYONair management had much more operational influence over FlyNYON contract flights.
Safety controls – NYONair did not have a formal safety structure and personnel did not have any formal safety training. NYONair’s lead pilot was appointed as their safety officer, although he did not have the authority to enforce safety-related policies. Liberty pilots did not have their own pilot safety meetings, and only their new safety officer represented the pilots at NYONair pilot and management meetings. The NYONair CEO made or heavily influenced all safety-related decisions, often disregarding the concerns of Liberty pilots.
Liberty had a safety director who left the company in October 2017. A new safety officer was in place in January 2018; however, he stated his position was informal and he had no training for his role. He reported directly to Liberty's chief pilot instead of management.
Neither company had a Safety Management System (SMS) in place, nor a formal safety program of any type. Investigators concluded that "ineffective safety management at both Liberty and NYONair resulted in a lack of prioritization and mitigation of foreseeable risks."
Flawed Assumptions
Safety harnesses – The operator apparently assumed that passengers could easily and quickly egress the helicopter in an emergency by releasing themselves by disconnecting the carabiner or by cutting the harness. It was further assumed the provided cutting tool would be effective in cutting the harness, if required. In this accident, none of the tethered passengers were able to free themselves for egress.
Helicopter flotation system – This FAA-approved flotation system was installed with a Supplemental Type Certificate (STC). Because the system was certified, it was assumed that when the system is installed and maintained as directed, it functions as designed. The FAA's certification review of the emergency flotation system design installed on the accident helicopter did not identify the manufacturer’s omission of an activation handle pull-force limitation. This led to the assumption that there were no limitations to installation routing or pull force limitations. There were no maintenance requirements or specifications to check or verify pull forces.
The pilot assumed that pulling the activation lever would activate the flotation system and keep the helicopter upright in the water. It appeared to the pilot that the inflation process was proceeding correctly and floats on both sides were inflating.
There was a certification assumption that only one of the two bottles of compressed nitrogen would sufficiently and evenly inflate all floats on the left and right skids to provide the necessary buoyancy to keep the helicopter upright in the water. The accident aircraft was unable to remain upright in the water when only one bottle discharged and the floats inflated asymmetrically. In post-accident testing, investigators verified that one bottle did not provide enough inflation to achieve the buoyancy and stability needed to keep the helicopter upright.
Unintended Effects
The use of a tether/harness for passenger safety resulted in unintentional engine shutdown when the tether was caught on and activated the FSOL.
The use of a tether/harness system to ensure passengers did not fall out of the helicopter was of complexity and design, making it difficult to egress the helicopter quickly in an emergency.
Columbia Helicopters CH-47D, ROTAK Helicopter Services, N388RA, North Fork, ID, July 21, 2022
A Columbia Helicopters CH-47D used for public firefighting operations crashed. The helicopter was hovering and preparing to load a water bucket from the Salmon River. Video evidence from the ground showed the yaw rotation swiftly increasing to the left as it descended and then impacted the river. The two occupants on board were fatally injured. Investigations focused on a crewmember iPad which appeared to have fallen into the anti-torque pedals. A damaged iPad was recovered. Further testing showed the iPad could have been wedged between the co-pilot’s left pedal and heel slide support assembly. Gouge marks on the iPad lined up with the pedal and heel support points of contact. Tests also showed the co-pilot would not be able to reach low enough to retrieve or dislodge the iPad from the pedal area.
NTSB accident report: CEN22FA331
Technical Related Lessons
Pilots and operators need to be aware of and prepare for external influences (e.g., passenger movement, shifting cargo, safety restraints, etc.) inadvertently actuating flight-critical, pilot-operated controls. (Threat Category: System/Component Failure or Malfunction (non-powerplant))
- The controls met the 14 CFR 27.1189(b) regulation to guard against inadvertent operation of each fuel shutoff.
- Optional STC modifications are available for various aircraft mission configurations that provide some protection from external influence in actuating the controls.
- In this accident, it was determined by investigators that the fuel shutoff lever (FSOL) was inadvertently manipulated by a passenger's tether that had become entangled in the lever and was pulled taut as he moved about in the seat.
Flotation systems need to be designed and installed for easy, sufficient, and reliable activation to keep the aircraft stable and upright on water for potential evacuation. (Threat Category: System/Component Failure or Malfunction (non-powerplant))
- Although it was approved by the FAA, the STC kit did not specify pull forces required to ensure correct operation, which would have enabled maintenance to determine if the system was installed and rigged correctly.
- The STC kit did not specify how to activate the system, such as two fingers, single hand, etc., nor did it specify a way for the pilot to verify the system had activated correctly.
- The pilot and maintenance community developed their own assumptions and cues of what constituted a successful deployment due to the lack of documented, specific pull forces and feedback cues or indications for the system.
- Although the FAA certified the flotation system, the design and engineering lacked sufficient guidance to fully test and maintain the system. Therefore, maintenance personnel did not have the direction or requirements needed to ensure the system would function as intended.
Common Theme Lessons
Occupants must be able to evacuate the aircraft easily and quickly, when necessary. (Common Theme: Flawed Assumptions)
- Per 14 CFR 27.785, helicopters must be equipped with safety restraints (safety belt and shoulder harness with a single-point release). However, these FAA-certified safety restraints basic to the accident aircraft were not a factor in this accident.
- In this accident, locking carabiners on the harnesses and floor were fastened in a manner not easily accessible to passengers. If passengers were unable to reach the locking carabiners, they were provided cutting tools to cut the harness or tether to enable egress in the event of an emergency. However, no instruction was given on how to use the provided cutting tool.