
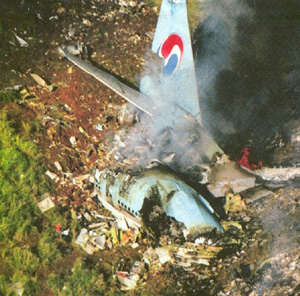
Boeing 747-300

Photo copyright Shotaro Shimizu - used with permission
Korean Airlines Flight 801, HL7468
Nimitz Hill, Guam
August 6, 1997
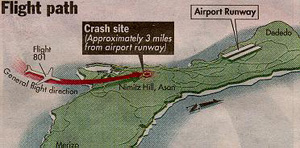
On August 6, 1997, during a non-precision approach to runway 06 left at A. B. Won Guam International Airport, Korean Airlines Flight 801 crashed at Nimitz Hill. Nimitz Hill is approximately three miles southwest of the airport, which is located at Agana, Guam. The airplane crashed into high terrain while conducting a non-precision approach. Of the 254 persons on board, 228 were killed. Twenty-three passengers and three flight attendants survived with serious injuries. The airplane was completely destroyed by impact forces and post-crash fire.
The National Transportation Safety Board (NTSB) determined that the probable cause of this controlled flight into terrain (CFIT) accident was the captain's failure to adequately brief and execute the non-precision approach and the first officer's and flight engineer's failure to effectively monitor and cross-check the captain's execution of the approach. Contributing to these failures were the captain's fatigue and Korean Air's inadequate flight crew training. Contributing to the accident was the Federal Aviation Administration's (FAA) inhibition, due to reliability concerns, of the minimum safe altitude warning system (MSAW) at Guam.
History of Flight
Flight 801, a Boeing 747-3B5B, departed Kimpo, Korea on August 6, 1997, at approximately 8:53 pm local time, enroute to Guam. The captain was the pilot flying (PF), and the first officer was performing as the pilot-not-flying (PNF). The captain had originally been scheduled for a flight to Dubai in the United Arab Emirates, but due to weather related delays on a previous flight, he had not acquired adequate rest for that flight, and so was reassigned to the shorter flight to Guam.
The flight to Guam was uneventful, and at 1:03 am, local time, the flight contacted the FAA's Guam Combined Center/Radar Approach Control (CERAP) controller. At initial contact, the flight was at an altitude of 41000 feet, approximately 240 nautical miles (nm) northwest of the NIMITZ VOR/DME. At 1:10 am, the controller instructed the flight to descend at their discretion to 2600 feet. Six minutes later, the captain began a crew briefing which included the radio frequencies for the instrument landing system (ILS) and VOR, which radios to tune to the various frequencies, and commented that since weather conditions were visual flight rules (VFR), that a go-around, if necessary, would be flown visually. He further noted that the glideslope was out of service, and as a result, the minimum descent altitude during the approach would be 560 feet, which corresponded to 304 feet above touchdown. Following this briefing, the flight began its descent. During the descent the cockpit voice recorder recorded several instances of the captain discussing crew scheduling and rest issues, including the comment that he was "really sleepy."

approximate location of crash site
While the flight descended, the flight crew discussed the weather being indicated on the weather radar, and that there appeared to be areas of heavy rain. The CVR recorded 6 minutes of conversation about the deteriorating weather, and the flight subsequently requested a deviation around concentrations of the heaviest weather.
At approximately 1:39 am, the controller issued instructions to intercept and join the localizer. At that time, the flight was descending through 2,800 feet, and wing flaps had been extended to 10 degrees. The first officer announced localizer capture, along with a comment about the glideslope that was largely unintelligible to the CVR. During this same time period, the controller cleared the flight for the ILS approach to runway 06 left, and informed the flight that the glideslope was unusable. The first officer acknowledged the clearance, but did not acknowledge that the glideslope was unusable. Almost immediately, the flight engineer asked whether the glideslope was working, and the captain responded affirmatively that it was. An unidentified voice recommended verifying that it was working, and then asked why it was working. The first officer responded, "not usable." After a few seconds, while the airplane was approximately 9 miles from the runway, the unidentified voice responded that the glideslope was incorrect. As the airplane approached 8 miles from the runway, the captain stated that since the glideslope was not "in good condition" that the flight needed to maintain 1440 feet. Just before 1:41 am, the CERAP controller handed the flight off to the control tower. The first officer contacted the tower as the airplane descended through 2000 feet at 6.8 nautical miles from the airport. At 1:41 am the tower cleared the flight to land, and the clearance was acknowledged by the first officer. No further communications with the tower were recorded.
As the first officer was acknowledging the clearance, the captain requested the flaps to be extended to 30 degrees in preparation for landing. At 1:41:31, the first officer called for the landing checklist. The captain said, "look carefully and set 560 feet" (the published minimum descent altitude). The first officer replied, "set," the captain called for the landing checklist, and the flight engineer began reading the checklist as the airplane descended through 1400 feet. As the airplane passed through 1400 feet, the ground proximity warning system (GPWS) altitude callout announced 1000 feet. At 1:40:46, the captain again asked if the glideslope was working, but received no response from other crew members. At this point, the captain requested that the windshield wipers be turned on. Once on, they remained on for the remainder of the flight.
At 1:41:53 the first officer again called for the landing checklist, and the flight engineer resumed reading the checklist items. At 01:41:59 as the airplane descended through 1100 feet, at 4.6 miles from the runway, a radio altitude callout of 500 feet was recorded on the CVR, followed about 2 seconds later by a remark from the first officer that the accident report characterized as "astonished", as though he was surprised by the altitude callout. As the airplane passed through 840 feet, the GPWS issued a "minimums minimums" annunciation, followed by a "sink rate" alert. The first officer commented that the sink rate of 1400 feet per minute was "ok."

- NTSB Docket Photo
At 1:42:19, as the airplane passed through 730 feet, the flight engineer called out, "200 feet", as the first officer said, "let's make a missed approach." One second later the flight engineer stated, "not in sight," and the first officer also said, "not in sight, missed approach." At 1:42:22, the flight data recorder indicated that the control column began increasing (nose up) at about 1 degree per second. The captain stated, "go around," and about 1 second later advanced the throttles. The nose up column deflection remained at about 1 degree per second. The radio altitude callouts began a sequential countdown of "one hundred...fifty....forty.....thirty.....twenty...." followed by impact on Nimitz Hill at an altitude of about 660 feet, and 3.3 nm from the airport. The CVR stopped recording at 1:42:32 am local time. An animation of the final minutes of the flight is available below.
Non-Precision Approach
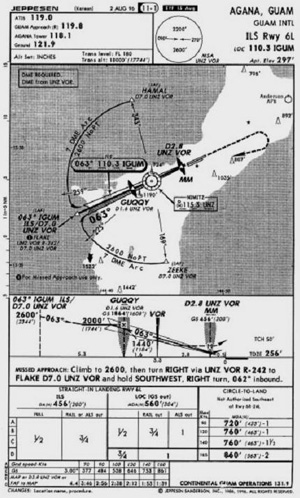
The Guam ILS 6L localizer-only (glideslope out) approach requires use of the NIMITZ VOR as a step-down fix between the final approach fix (FAF) and the runway, and DME to identify the step-down points. The DME is not collocated with the localizer transmitter (which is located at the airport), but is located at the VOR.
View Larger
The non-precision localizer-only approach requires the use of the localizer to obtain lateral guidance to the runway, the DME to identify the step-down points, and the VOR to identify the final step-down fix to the minimum descent altitude. According to the approach plate effective at the time, the airplane should cross the FLAKE initial approach fix (IAF) - located at 7 nautical miles, per the DME, from the VOR - at or above 2600 feet before reaching the outer marker, which is the FAF, located at 1.6 nautical miles from the VOR. Upon crossing the FAF, the procedure prohibits descent below 1440 feet until passing the VOR. The procedure calls for a descent to 560 feet, and the pilot is required to count up from less than 1 nautical mile DME as the airplane passes over the VOR, to 2.8 nautical miles DME, the published missed approach point and location of the middle marker. If a missed approach is not required, the airplane can continue its descent to the runway, located at 3.3 nautical miles from the VOR.
According to the accident report, in order to properly execute this approach, the captain's navigation receiver would have needed to be tuned to the localizer frequency, and the first officer's navigation receiver would need to be tuned to the VOR in order to acquire DME (distance) information for the FLAKE intersection, the outer marker, and the missed approach point, and allow identification of station passage over the VOR. Station passage over the VOR would be identified by a change in the TO/FROM indicator in the first officer's instruments from TO to FROM, and the instrument pointer on the first officer's DME indicator would have swung from pointing forward to pointing aft. Station passage would have also been indicated by a DME countdown to near zero followed by a countup as the airplane proceeded away from the VOR.
The investigation determined that the CERAP controller vectored flight 801 to join the localizer between the FLAKE intersection and the outer marker. Although at this point the flight was restricted to no lower than 2000 feet (until crossing the outer marker) the flight descended below 2000 feet about 1.9 nautical miles prior to reaching the outer marker. The approach further required that 1440 feet be maintained after passing the outer marker until passing the VOR. Flight 801 descended below 1440 feet about 2.1 nautical miles before reaching the VOR.

CVR recordings indicated that the captain was flying the airplane with the autopilot engaged during the approach. As the flight descended during the approach the captain twice commanded the entry of lower altitudes into the airplane's altitude selector before the airplane had reached the associated step-down fix. The accident report stated that after hearing the first officer (erroneously) call out that the airplane was approaching 1400 feet, as the airplane was passing 2400 feet at 5 nautical miles from the VOR, he directed the first officer to reset the altitude to 1440 feet, replacing the step-down altitude of 2000 feet before the autopilot had captured that altitude, or reached the outer marker where descent to 1440 feet would have been authorized. Finally, before the flight leveled at 1440 feet, and prior to reaching the VOR step-down fix, the captain instructed the first officer to set 560 feet, the minimum descent altitude, in the altitude selector.
The altitude selector provides the basis for aural annunciations and the autopilot's altitude capture functions. The investigation concluded that the captain's premature orders to reset the altitude selector indicated that he had lost awareness of the airplane's position along the final approach course. As a result of the captain's commanded input to the altitude selector, the autopilot continued to descend prematurely through the 2000 and 1440 foot intermediate altitude constraints. The CVR comments indicated no awareness by the captain that the airplane was descending prematurely below the required intermediate altitudes.
Weather Factors during the Approach
Weather data indicated that the weather during the time period before the accident was variable clouds and rain showers that increased in intensity as they moved over the higher terrain of the island. NTSB interviews with crews who flew into Guam before and after the accident indicated that the lights of the island were sometimes visible from as far away as 150 nautical miles. CVR data indicated that flight 801 visually acquired the island about 16 minutes before the accident.

The investigation concluded that flight 801 was likely to have initially encountered variable to scattered cloud layers below 5000 feet during final approach. Ground lights were likely to have been occasionally visible along the coastline, and it was probable that only scattered clouds existed below the airplane in the vicinity of FLAKE intersection.
Radar indicated a concentration of heavy rain about 4 nautical miles southwest of the airport, along the approach corridor. As the airplane descended through 2,000 feet, it would have entered clouds and experienced rain of increasing intensity that became very heavy as the airplane neared the outer marker. This would have coincided with the captain's request to turn on the windshield wipers. The NTSB concluded that flight 801 likely exited a rain shower before the accident, but was not able to visually acquire the airport because of another shower located between Nimitz Hill and the airport.
The NTSB noted that a month prior to the accident, the captain had flown into Guam, and executed a routine ILS approach in good visibility. For the accident flight, the most current weather information available indicated that visual conditions existed at the airport. Korean Air's airport familiarization video which the captain and first officer had viewed the previous July noted that weather conditions at Guam allowed visual approaches most of the year, and that in the event of instrument meteorological conditions, positive guidance would be provided by air traffic control. The NTSB concluded that this may have caused the captain to anticipate a visual approach.
The NTSB noted that the captain's landing briefing included references to his expectation of a visual approach, as well as an abbreviated briefing for the localizer approach. The NTSB concluded that his expectation of a visual approach was a factor in his incomplete briefing of the localizer approach, and contributed to the accident.
Air Traffic Control
Investigators evaluated the performance of the CERAP and tower controllers to establish if their performance had contributed to the accident. The investigation found three controller deviations. When he cleared the flight for the approach, per procedure, the CERAP controller should have provided a position advisory at the time he granted the clearance. The NTSB concluded that if a position report had been provided, the flight crew may have been prompted to cross check their position, improving their situational awareness. The NTSB also stated that the controller did not provide a weather update, including the presence of a rain shower between the flight and the airport, awareness of which may have influenced their decision making.
According to the NTSB, the CERAP controller also failed to monitor the flight after the frequency change to the control tower. Had he been monitoring the flight , he might have observed flight 801 disappear on final approach, or may have noticed the approach path warning (low altitude alert) which began about 6 seconds prior to impact.

Further, if the CERAP controller had continued to monitor the flight, the NTSB stated that he may have seen the airplane's premature descent, and could have provided an alert to the flight crew. His radar display would have shown the airplane descending through 2000 feet while still 7 miles from the airport, and would further have seen the airplane crossing the outer marker 800 feet lower than the established crossing altitude of 2000 feet.
The NTSB concluded that the CERAP controller's performance was substandard in that he failed to provide the flight crew with a position advisory when he cleared the flight for the approach, inform the flight crew and tower controller of rain showers on the final approach path, and monitor the flight after handoff to the tower.
In addition, Guam radar facilities had been equipped, since February, 1995 with a minimum safe altitude warning system (MSAW) intended to warn controllers of aircraft descents below minimum safe altitudes during approaches. The system had originally been operative to provide altitude alerts within a 54 nautical mile ring around the radar antenna. Due to the generation of a high volume of nuisance alerts, the system had been inhibited, and at the time of the accident was capable of generating a low altitude alert only in a 1 mile-wide band between 54 and 55 nautical miles. Flight 801 crashed in an area that would have been covered had the MSAW been operative. The investigation concluded that the MSAW would have provided a 64 second warning, allowing the controller adequate time to warn the flight, and perhaps avert the accident.
Flight Crew Training and Crew Resource Management (CRM)
The NTSB examined Korean Airline's training programs to determine if there were any causal links to the accident, especially with respect to flight crew performance on the accident flight. In 747 training, the airline conducted 10 4-hour simulator sessions consisting of flight maneuvers, including various types of approaches. The only non-precision approach practiced in the simulator sessions was a DME/VOR approach to runway 32 at Kimpo Airport. The training approach was significantly different, and less complex than the approach into Guam, and did not require a countdown, and then countup procedure after passing over the DME station, as did the Guam approach. The Safety Board expressed concern that the repeated presentation of a single non-precision approach in training exercises did not provide sufficient training in non-precision approaches. Further, the NTSB believed that the repetitive nature of training for non-precision approaches limited pilots' opportunity to understand and practice flying techniques necessary to perform different kinds of non-precision approaches, and limits ability to successfully apply these techniques to novel situations or unusual approach configurations that can be encountered in line operations, such as the Guam approach. The Safety board concluded that Korean Air's execution of non-precision approach training was ineffective, and contributed to the deficient performance of the crew of flight 801.

The NTSB stated that from CVR evidence, the crew was confused about, and did not react to a series of GPWS alerts during final approach which should have caused them to assess their position on the approach, and execute a missed approach. The flight crew concentrated on determining the operational status of the glideslope indication, to the detriment of proper execution of the non-precision approach. Further, having conducted an inadequate approach briefing, the crew was unprepared to react properly to the GPWS warnings, and other indications that the approach was not progressing safely. Loss of situational awareness led to the premature descent, which went unchallenged by the other members of the flight crew. Proper execution of CRM practices, and proper monitoring of the approach by the non-flying pilot could have averted the accident.
Flight Crew Fatigue
The accident occurred after midnight based on the crew's home time zone, a period which research has shown is often associated with degraded alertness and a higher probability of error and accidents. The accident report also stated that the time of arrival at Guam was also several hours after the captain's normal bedtime, and a time at which his body would be primed for sleep. During the flight, the captain had made comments about being tired, which investigators believed could have been indicative of symptoms that could lead to significant performance degradation. On the day of the accident, the captain had been awake for 11 hours at the time of the accident. The Safety Board has found 11 hours since awakening to be significant, and is a time associated with greatest errors. Based on the evidence discovered during the accident investigation, the NTSB determined that the captain was fatigued, which degraded his performance and contributed to his failure to properly execute the approach.

The NTSB issued 36 findings discussing:
- The weather conditions at the time of the accident
- Korean Airlines flight crew procedures
- Crew resource management and crew situational awareness
- The challenges of flying a non-precision approach into Guam
- Airline crew training
- The status of the Guam airport radar facilities
- And various findings related to the search and rescue operations following the accident
The findings, including the accident probable cause are available at the following link: (Accident Findings). The complete accident report is available here: (NTSB Accident Report)
The NTSB issued 15 recommendations: 12 to the FAA, two to the Governor of the Territory of Guam, and one to the Korean Civil Aviation Bureau. The recommendations to the FAA covered a wide range of subjects, while the recommendations to the Governor of the Territory of Guam addressed territorial emergency responses and emergency response agency coordination. The recommendation to the Korean authorities addressed training associated with the complexities of non-precision operations into Guam. The complete text of the recommendations is available at the following link: (NTSB Recommendations)
14 CFR 129.1 Applicability.
14 CFR 129.13 Airworthiness and registration certificates.
14 CFR 129.15 Flight crewmember certificates.
14 CFR 129.17 Radio equipment.
14 CFR 129.19 Air traffic rules and procedures.
14 CFR 129.21 Control of traffic.
14 CFR part 129 governs the operations of foreign air carriers into the United States or its territories. In order to operate into U. S. territory, a foreign airline must operate per the requirements of part 129. The FAA will assign a principal operations inspector to the airline and approve an operations specification for that carrier to be applicable when operating in U.S. airspace. Part 129 generally specifies the requirements for airworthiness for aircraft, navigation, and communication capabilities and air crew qualifications.
A section in the accident report cites a study conducted by the Airline Pilot's Association (ALPA), which indicated that airline crews conduct only one to three non-precision approaches per year and practice these approaches in a simulator just as infrequently. ALPA concluded that the risk associated with this inherently less safe type of approach is compounded by the infrequency of flight crew exposure and practice. The ALPA study stated that most non-precision approaches are presented as a series of step-down altitudes which may be satisfactory for light, slow, maneuverable aircraft, but are unacceptable for transport category aircraft. ALPA further stated that step-down altitudes are, in fact, contrary to the concept of a stabilized approach, as they require multiple pitch and thrust changes to fly the approach as specified. ALPA stated that approach charts and procedures should be modified to provide the information necessary to conduct stabilized approaches without explicit vertical guidance.
Further, in testimony during the accident hearings, an airline captain, who had been a member of both an industry task force aimed at landing accident reduction and a second task force aimed at CFIT awareness, testified about the factors involved in CFIT accidents. He testified that five of six CFIT accidents in 1996 and 1997 occurred during non-precision approaches, and that from 1988 to 1997 one half of the commercial CFIT accidents were during step-down approaches, even though most of the accident airplanes were equipped with distance measuring equipment, which should have aided in determining the step-down points during the approach.
The captain testified that, according to the accident data, the chances of a CFIT accident during a non-precision approach is five times greater than during a precision approach. The captain stated that non-precision approaches are generally much more complex than precision approaches because they are less familiar to pilots, are more prone to error, and require more comprehensive briefings. He further testified that non-precision approaches need particularly careful and accurate monitoring, and that it is possible with complex step-down, procedures for steps to be missed or taken out of order. He recommended eliminating step-down non-precision approaches. He further advocated much more carefully managed airplane crews and checklists because many CFIT accidents occur when the crew is preoccupied or distracted by other tasks.
- Premature descent during a non-precision approach, resulting in controlled flight into terrain
- Flight crew fatigue leading to loss of airplane position awareness relative to terrain
- Improper execution of complex non-precision approach
- Occurrence of CFIT accidents, such as Korean Air Flight 801 would be mitigated by the installation of GPWS systems, and that flight crews would respond properly, and in a timely manner upon actuation of a GPWS alert
- Flight crews would properly execute a complex non-precision approach at night in adverse weather
TWA Flight 514, Boeing 727-231, December 1, 1974, near Berryville, Virginia
While on descent for landing at Dulles International Airport in Washington, D.C., TWA Flight 514, a Boeing 727-231, impacted terrain about 25 miles from the airport. All 85 passengers and seven crew members were killed, and the aircraft was destroyed. The flight was descending for a VOR/DME approach into Dulles in instrument meteorological conditions (IMC) and had descended to 1,800 feet approximately 40 miles from the airport. The NTSB determined that the descent to 1,800 feet had occurred prior to the aircraft reaching a point in the approach where a minimum altitude of 1,800 feet would have been safe. The NTSB further determined that the crew's decision to descend was "a result of inadequacies and lack of clarity" in air traffic control procedures and a misunderstanding between pilots and controllers regarding each other's responsibilities during terminal operations and in IMC conditions. However, primary responsibility for the accident was placed on the pilots for having descended to an unsafe altitude.
See accident module
American Airlines Flight 965, B-757, N651AA, December 20, 1995, Near Cali, Colombia
On the evening of December 20, 1995, at approximately 2142 Eastern Standard Time (equivalent to Cali, Colombia local time), American Airlines Flight 965 crashed into high terrain during approach to Alfonso Bonilla Aragon International Airport, Cali, Colombia. Of the 163 people on board only four survived. The weather conditions that night were relatively clear skies and light surface winds with no moon.
The airplane involved in this accident, a Boeing 757, was equipped with cathode ray tubes (CRT), or "glass cockpit" technology, including screens which display flight path and navigation information, engine information, and a Flight Management System (FMS). A Ground Proximity Warning System (GPWS) was also installed and functioned normally at the time of the accident.
The investigation concluded that this accident was attributed to flight crew human error involving navigational and crew resource management lapses. This Controlled Flight Into Terrain (CFIT) accident became the catalyst for requiring the installation of terrain awareness and warning systems (TAWS) in transport airplanes.
See accident module
Korean Airlines
Following the accident, no airworthiness directives were issued to mandate corrective actions for the 747 or other model airplanes. However, a number of actions aimed at correcting other identified problems were initiated. Korean authorities ordered Korean Air to suspend 138 flights per week on ten of its domestic routes for six months. Additional administrative actions were also taken. Captain qualification requirements were increased for large aircraft, including the 747. First officers were prohibited from serving their initial first officer assignment on large aircraft, such as the 747; simulator training and line-oriented flight training (LOFT) were increased; and special simulator training for adverse weather conditions was initiated.
Following these requirements, Korean Airlines also undertook a two-year safety initiative, including changes in pilot training and maintenance operations. The airline announced that it intended to accomplish a number of objectives:
- Installation of enhanced GPWS in all new aircraft, and an upgrade of TCAS on all airplanes
- Safety awareness training to all flight crewmembers
- Aircraft-specific safety training for all flight crews, including an expanded CFIT awareness program
- Development of a safety alert system, gathered from throughout the Korean Air system, aimed at identifying trends and developing accident prevention strategies
- Development of simulator scenarios that reflect a variety of situations that may be encountered operationally, including operations from different airports, TCAS avoidance maneuvers, and GPWS escape maneuvers
- Standardization of pilot callouts, improvement of checklists, and enhancement of pilots' knowledge of local terrain
- CRM and LOFT training for all flight crew members aimed at efficient and effective communication on the flight deck and in the cabin
Korean Air also implemented a five-point Immediate Action Plan, implementing safety measures that were designed to minimize exposure to risk, elimination of known hazards, and curtailment of operation under circumstances where there may be reduced safety margins. Further, the airline adopted duty time rules that were similar to the duty time standards established under FAA's 14 CFR part 121 requirements. The indicated goal was to achieve a standard of 80 hours of flight time per month for crew members, and to implement an automated crew scheduling system to monitor training, currency, and compliance with duty time requirements. Finally, the airline implemented an extensive revision of operational manuals in order to achieve company operational standardization.
Minimum Safe Altitude Warning (MSAW)
As a result of this accident, on August 15, 1997, the FAA ordered testing and recertification of MSAW. The FAA reported that 190 of the 192 MSAW sites were confirmed to be working properly. The two facilities where the software was not functioning properly were corrected, and the functions were recertified. Further, the FAA created special teams of experts to completely examine all the site adaptation parameters for all 192 MSAW locations throughout the United States. The FAA directed air traffic control managers at all locations to document and report and anomalies.
In addition, the FAA conducted a fact-finding review of MSAW equipment and operational procedures at ten facilities. The review included a survey of 105 air traffic personnel and 33 airway facilities personnel. As a result of the review, a number of FAA internal recommendations were made:
- Establishment of a comprehensive training program to provide a basis for entry level and periodic refresher training in the operation and maintenance of MSAW and a certification process for recipients of training
- Uniform site adaptation/system parameters should be established for MSAW operation
- Periodic evaluation of MSAW equipment
- Configuration management of all software and centrally located and controlled documents
The FAA further developed an agency plan for corrective actions for the MSAW system, and a central oversight process for the MSAW program, including flight checks, equipment certification, and management and control for MSAW software modifications.
Terrain Awareness and Warning System (TAWS)
In March 2000, the FAA issued 14 CFR 121.354 requiring the installation of TAWS on the U.S. airline fleet by March 2005. Following this accident and an American Airlines 757 accident in Cali, Colombia in 1995, the FAA determined that installation of TAWS would reduce the incidence of CFIT accidents. For airplanes operated under 14 CFR Part 121, the rule was made applicable to all turbine powered airplanes. For those operated under 14 CFR Parts 91, 125, 129, and 135, the rule was made applicable to all turbine-powered airplanes with six or more passenger seats.
The complete text of the rule is available here: (14 CFR 121.354)
Airplane Life Cycle:
- Operational
Accident Threat Categories:
- Crew Resource Management
- Flight Deck Layout / Avionics Confusion
- Incorrect Piloting Technique
Groupings:
- Controlled Flight Into Terrain
- Approach and Landing
- Automation
Accident Common Themes:
- Organizational Lapses
- Human Error
Organizational Lapses
The NTSB stated in the accident report that Korean Air's training syllabus for non-precision approaches was limited and employed simulator training using a relatively non-complex approach into Kimpo, Korea. The safety board expressed concern that the repeated presentation of a single non-precision approach in training exercises did not provide sufficient overall training in non-precision approaches. Further, the NTSB believed that the repetitive nature of the airline's training for non-precision approaches limited pilots' opportunity to understand and practice flying techniques necessary to perform different kinds of non-precision approaches. The safety board concluded that Korean Air's execution of non-precision approach training was ineffective and contributed to the deficient performance of the crew of Flight 801.
Human Error
The NTSB concluded that the flight crew had lost situational awareness and were unsure of their location on the approach relative to the runway and surrounding terrain. During the complex step-down approach, the captain repeatedly instructed the first officer to reset the next lowest altitude prematurely, causing the flight to descend below the minimum descent altitudes for critical approach flight segments. The flight crew concentrated on whether or not the glideslope, which was out of service, was actually operational to the detriment of execution of the approach. They ignored repeated GPWS alerts that the flight was too low, and having conducted an incomplete approach briefing, were not adequately prepared to assess the situation and respond appropriately by executing a missed approach.
TWA Flight 514, Boeing 727-231, December 1, 1974, near Berryville, Virginia
While on descent for landing at Dulles International Airport in Washington, D.C., TWA Flight 514, a Boeing 727-231, impacted terrain about 25 miles from the airport. All 85 passengers and seven crew members were killed, and the aircraft was destroyed. The flight was descending for a VOR/DME approach into Dulles in instrument meteorological conditions (IMC) and had descended to 1,800 feet approximately 40 miles from the airport. The NTSB determined that the descent to 1,800 feet had occurred prior to the aircraft reaching a point in the approach where a minimum altitude of 1,800 feet would have been safe. The NTSB further determined that the crew's decision to descend was "a result of inadequacies and lack of clarity" in air traffic control procedures and a misunderstanding between pilots and controllers regarding each other's responsibilities during terminal operations and in IMC conditions. However, primary responsibility for the accident was placed on the pilots for having descended to an unsafe altitude.
See accident module
Continental Jet Link, Embraer EMB-120RT, N24706, April 29, 1973, Pine Bluff, Arkansas
The airplane crashed during a forced landing and runway overrun at a closed airport. No injuries occurred. The accident occurred on the third day of a 3-day sequence, and the accident flight was the seventh and last scheduled flight of the day. During climb, the autopilot was engaged in pitch and heading modes contrary to company policy. The airplane decelerated during the climb and eventually stalled while in instrument meteorological conditions. An initial stall recovery was made at 6,700 feet, but due to improper recovery techniques, a second stall occurred, and recovery was at 5,500 feet. The left propeller shed three blades and the left engine cowl separated, resulting in the requirement to shut down the left engine. Level flight could not be maintained, and a forced landing was made. Due to controllability problems, the turn to align the airplane with the runway was overshot, and the airplane landed above the normal approach speed and with only 1,880 feet of runway remaining. The runway was wet, and hydroplaning conditions caused the airplane to skid off the end of the runway.
The NTSB determined that the cause of the accident was "the captain's failure to maintain professional cockpit discipline, his consequent inattention to flight instruments and ice accretion, and his selection of an improper auto flight vertical mode, all of which led to an aerodynamic stall, loss of control and a forced landing. A factor contributing to the accident was fatigue induced by the flight crew's failure to properly manage provided rest periods."
American International Airways Flight 808, McDonnell Douglas DC-8-61, N814CK, August 16, 1993, Guantanamo Bay, Cuba
While on approach to Guantanamo Bay, Cuba, the airplane collided with level terrain approximately one-quarter mile from the approach end of the runway, after the captain lost control of the airplane. The airplane was destroyed by impact forces and post-crash fire. The three crewmembers (the only occupants) received serious injuries.
According to the accident report, the flight crew had been on duty for 18 hours and had flown approximately nine hours. The captain did not recognize deteriorating flightpath and airspeed conditions because of his preoccupation with locating a strobe light on the ground. The flight engineer made repeated callouts regarding low airspeed during the approach. The captain initiated a turn on final approach at a speed below the prescribed approach speed and using bank angles exceeding 50 degrees. The airplane subsequently stalled, and control was lost. The investigation concluded that the substandard piloting performance may have reflected the debilitating influences of fatigue.
The safety board determined the probable cause of the accident was the impaired judgment, decision-making, and flying abilities of the captain and other flight crewmembers because of the effects of fatigue; the captain's failure to properly assess the conditions for landing and maintaining vigilant situational awareness of the airplane while maneuvering onto final approach; his failure to prevent the loss of airspeed and avoid a stall while in the steep bank turn; and his failure to execute immediate action to recover from a stall. Additional factors contributing to the cause of the accident included the inadequacy of the flight-time and duty-time regulations applied to 14 CFR Part 121 supplemental air carriers, international operations, and the circumstances that resulted in the extended flight and duty hours and fatigue of the flight crewmembers.
American Airlines Flight 965, B-757, N651AA, December 20, 1995, Near Cali, Colombia
On the evening of December 20, 1995, at approximately 2142 Eastern Standard Time (equivalent to Cali, Colombia local time), American Airlines Flight 965 crashed into high terrain during approach to Alfonso Bonilla Aragon International Airport, Cali, Colombia. Of the 163 people on board only four survived. The weather conditions that night were relatively clear skies and light surface winds with no moon.
The airplane involved in this accident, a Boeing 757, was equipped with cathode ray tubes (CRT), or "glass cockpit" technology, including screens which display flight path and navigation information, engine information, and a Flight Management System (FMS). A Ground Proximity Warning System (GPWS) was also installed and functioned normally at the time of the accident.
The investigation concluded that this accident was attributed to flight crew human error involving navigational and crew resource management lapses. This Controlled Flight Into Terrain (CFIT) accident became the catalyst for requiring the installation of terrain awareness and warning systems (TAWS) in transport airplanes.
See accident module
Philippine Airlines Flight 110, Airbus A330, December 16, 2002, Agana, Guam
On December 16, 2002, at approximately 0135 local time, an Airbus A330, Philippine registration F-OHZO, operating as Philippine Airlines Flight 110 (PAL110), struck power lines while executing a localizer-only Instrument Landing System (ILS) approach to runway 6L at A.B. Pat Won Guam International Airport, Agana, Guam (GUM). Instrument meteorological conditions prevailed during the approach. Following a ground proximity warning system (GPWS) alert, the crew executed a missed approach and landed successfully after a second approach to the airport. The aircraft remained on the ground at Agana until departing at 0515 to return to Manila as PAL Flight 111. According to information provided by Philippine Airlines, after arriving at Manila the aircraft was inspected and found to have minor damage to the fuselage and landing gear. There were no reported injuries to passengers or crew. As airplane damage was minor, and no injuries were sustained by passengers or crew, this was classified as an incident by the NTSB. The NTSB incident report is available at the following link: (A330 Incident Report) Note: Portions of this report were originally arranged in a tabular format that was not retained in this copy.
Technical Related Lessons
Complex approaches, especially when executed at night and/or in inclement weather, or where terrain is a factor, must be carefully and fully briefed, and associated procedures and approach constraints must be followed and monitored to avoid CFIT accidents. (Threat Category: Crew Resource Management)
- The investigation concluded that the flight crew did not conduct a thorough briefing prior to beginning the approach, and that during the approach the crew lost situational awareness relative to their location on the approach. The captain continually and prematurely ordered increasingly lower altitude selections, resulting in an approach profile that was consistently below the minimum required safe altitude. Further, though the crew was aware that the glideslope was inoperative, intermittent indications on the associated instruments caused some confusion among that crew as to whether or not the glideslope might be active to the detriment of proper monitoring of the Localizer-only approach that was being executed. The intermittent fixation on the glideslope indications contributed to a delayed awareness that the airplane was too low and late initiation of a go-around.
The performance of early generation ground proximity warning systems (GPWS) exhibited inherent limitations that, under certain operational conditions, did not consistently provide cues to the flight crew in order to prevent controlled flight into terrain accidents. Current terrain avoidance warning systems (TAWS) using graphic displays and terrain databases substantially enhances the ability to maintain terrain awareness and avoid CFIT accidents. (Threat Category: Flight Deck Layout/Avionics Confusion)
- During the investigation the NTSB conducted a number of simulations using enhanced GPWS (now known as TAWS) and concluded that if flight 801 had been equipped with TAWS, an aural "CAUTION TERRAIN" warning and a yellow visual terrain depiction on the weather radar display would have been provided about 60 seconds before impact. An aural "TERRAIN TERRAIN" and "PULL UP" warning and a red visual terrain depiction would have been issued about 45 seconds before impact and would have sounded continuously until completion of a successful escape maneuver or impact.
A decision to go-around should be made without delay when missed approach conditions are present (failure to visually acquire the runway, reaching minimum descent altitude, etc.). Once the go-around decision has been made, flight control inputs and engine thrust increase should be conducted immediately. (Threat Category: Incorrect Piloting Technique)
- The NTSB concluded that the first officer and flight engineer responded to GPWS annunciations of low altitude above the ground, and the first officer properly called for a missed approach. It was also concluded that once the go-around decision had been made, the captain's control inputs were not immediate, and not of sufficient magnitude to properly initiate the go-around or arrest the existing sink rate. The captain's failure to react in a timely manner to the GPWS "minimums" annunciation, and his further failure to immediately initiate a go-around when prompted by the first officer, led to the accident.
Common Theme Related Lessons
Deviation from assigned or required procedures, especially when those procedures are complex or not routinely practiced, is accompanied by a high potential for error, and can lead to crew confusion. Procedures need to be closely monitored during their execution to avoid errors or loss of situational awareness. (Common Theme: Human Error)
- The investigation concluded that the approach had been inadequately briefed by the captain. Further, during the approach the first officer erroneously called out that the flight had reached an altitude 1,000 feet lower than had actually been achieved. The captain then ordered the next lowest step-down altitude in the approach to be set, and before passing the next radio fix, inappropriately commanded the final minimum altitude to be set. This allowed the airplane to descend prematurely and to remain significantly below the specified minimum safe altitudes for several segments of the approach. Coupled with the crew's confusion over intermittent glideslope signals, approach monitoring deteriorated, and the airplane was allowed to descend into the ground well short of the runway. The NTSB further commented on the crew's loss of situational awareness as having been a contributing factor in the accident.