
Boeing 727-231

Photo copyright Kjell Nilsson - used with permission
Trans World Airlines Flight 514, N54328
Mt. Weather, Virginia
December 1, 1974
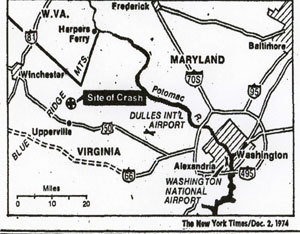
While on descent for landing at Dulles International Airport in Washington, D.C., TWA Flight 514, a Boeing 727-231, impacted terrain about 25 miles from the airport. All 85 passengers and seven crew members were killed, and the aircraft was destroyed. The flight was descending for a VOR/DME approach into Dulles, in instrument meteorological conditions (IMC), and had descended to 1,800 feet approximately 40 miles from the airport. The NTSB determined that the descent to 1,800 feet had occurred prior to the aircraft reaching a point in the approach where a minimum altitude of 1,800 feet would have been safe. The NTSB further determined that the crew's decision to descend was "a result of inadequacies and lack of clarity" in air traffic control procedures and a misunderstanding between pilots and controllers regarding each other's responsibilities during terminal operations and in IMC conditions. However, primary responsibility for the accident was placed on the pilots for having descended to an unsafe altitude.
History of the Flight

Photo copyright Steve Williams - used with permission
Trans World Airlines Flight 514 was scheduled from Indianapolis, Indiana to Washington, D.C., with an intermediate stop in Columbus, Ohio. The early flight segments were uneventful. Shortly after takeoff from Columbus, the flight was informed that no landings were being made at Washington National Airport (the intended destination) due to heavy snow in the region, and flights to that airport were either being held or diverted to Dulles International Airport. Following a radio discussion with the TWA dispatcher in New York, the captain decided to divert to Dulles. Shortly thereafter, the flight began a series of descents in preparation for the approach into Dulles. The flight was cleared to descend to 23,000 feet and instructed to cross a point 40 miles west of Fort Royal (the initial approach fix, or IAF) at that altitude. At this point, control of the flight was transferred from the Cleveland Air Route Traffic Control Center (ARTCC) to the Washington ARTCC. During the time between amending their flight plan to divert to Dulles and the transfer of control to the Washington ARTCC, the flight crew discussed the approach to runway 12 at Dulles, the navigational aids, and the runways. Following this discussion, the captain turned the flight controls over to the first officer.
Copyright New York Times
Upon initial contact with the Washington ARTCC, the controller acknowledged that he knew the flight was proceeding to Dulles, and the CVR recorded a crew conversation about the possible approach routings that could be anticipated for conducting a VOR/DME approach to runway 12 at Dulles. The discussion included the possibilities of proceeding via the Fort Royal VOR, via the Martinsburg VOR, or receiving a "straight-in" clearance to runway 12. After verifying the position of the airplane, the controller issued instructions to intercept the 300 degree radial of the Armel VOR, and to cross a point 25 miles northwest of Armel at 8,000 feet. These instructions were slightly different than those of the Cleveland ARTCC controller. At this point, the crew again discussed the approach procedure, including the Round Hill intersection, the final approach fix and details of the airport. During this same time period, the flight had been incrementally descending per the controller's instructions, and was cleared to descend to and maintain 7,000 feet. Upon reaching 7,000 feet, the flight reported and immediately received the instruction, "TWA 514, you're cleared for a VOR/DME approach to runway 12." The clearance was acknowledged, and the captain commented to the first officer, "Eighteen hundred is the bottom." The first officer then commented, "Start down." The investigation concluded that the decision to descend to 1,800 feet was based on the crew's misinterpretation of the approach plate, which contained discrepant information, and contributed to the conclusion that 1,800 feet was a safe altitude. In fact, 3,400 feet was specified as the minimum descent altitude on the approach plate. The investigation further concluded that the crew's decision to descend to 1,800 was the principal error leading to the crash. At the initiation of this final descent, the flight was approximately 44 miles from the airport. The descent to 1,800 feet was conducted over the next 20 miles, leveling at 1,800 feet just before impact with Mt. Weather, located about 25 miles from the airport. View TWA Flight 514 Flightpath Animation below:
Dulles International Airport Facilities

Photo copyright Sid Star - used with permission
Dulles is equipped with three primary runways, 12/30, 1L/19R, and 1R/19L. The north-south runways are 11,500 feet long, and runway 12/30 (the intended runway for Flight 514) is 10,000 feet long. Instrument landing system (ILS) approaches are available for the north-south runways. Runway 12 is served by a VOR/DME approach. Additionally, a surveillance radar approach is available to all runways.

(Co-located VOR and military TACAN).
DME Transmitter is the tower to the left of the photo
An ILS provides vertical and lateral guidance to the intended runway, and provides the capability to land when visibility is low. Depending on the accuracy of the ILS facility, a manual approach and landing can be accomplished with ceilings typically as low as 100 feet, and visibility of just a half mile. If an airplane is equipped with an automatic landing system, and certain other facility accuracy and reliability requirements are met, landings can potentially be performed when ceilings and visibility are zero.
A VOR (Very high frequency Omni-Range) provides navigational information to/from a VOR facility, sometimes located at an airport, by providing a bearing (heading) to/from the facility. VOR facilities generally also provide distance information to/from the facility. By flying specific bearings to/from the VOR facility, an airplane can navigate to fly over an airport, but vertical guidance from a controller is still necessary to properly position the airplane at the initial approach fix, allowing safe completion of the approach. Since the final phases of the landing must be conducted via visual reference to the runway, the ceiling and visibility requirements are necessarily higher than those for an ILS approach.
Approach Procedures
Upon establishing communications with the Washington ARTCC, the flight was issued a heading change from 100 degrees to 090 degrees in order to better position the flight to intercept the inbound course. At the same time, the flight was issued instructions to intercept the 300 degree radial to the Armel VOR, to cross a point 25 miles northwest of Armel, and maintain 8,000 feet. At this time the flight was also informed that they would be making a VOR/DME approach to runway 12. Shortly after this contact, the flight was cleared to 7,000 feet and told to contact Dulles approach control.
On initial contact with Dulles approach control, the controller confirmed that a VOR/DME approach to runway 12 was expected. Five seconds after this communication, the flight received the clearance for the approach, and decided to initiate a descent from 7,000 to 1,800 feet, based on earlier flight deck conversations about the minimum descent altitude. The controller did not explicitly clear the flight to begin the descent, but approach procedures at the time would have allowed descent to the specified minimum descent altitude. The minimum descent altitude should have been recognized as 3,400 feet. The flight was approximately 40 miles from the airport when it departed 7,000 feet.
During the descent from 7,000 feet, the captain noted that the approach plate specified a minimum altitude of 3,400 feet prior to reaching the Round Hill intersection. The flight was already below 3,400 feet, and had not yet reached Round Hill. A discussion ensued, concluding that because they had been cleared for the approach, the 3,400 foot altitude restriction did not apply, and a descent to 1,800 feet was appropriate. Shortly after leveling off at 1,800 feet, impact with Mt. Weather occurred.

- NTSB Docket Photo
In the official accident report, the National Transportation Safety Board (NTSB) discussed the air traffic control procedures and protocols for this type of approach. Historically, prior to a primarily radar environment and positive traffic control, especially during approach, flight crews were solely responsible for knowing the position of their aircraft. With the advent of radar-based traffic control, procedures became more dependent on information provided by the controller. The controller was able to "see" the airplane relative to its range and bearing to a specific location, and could provide heading information to prevent track convergence of controlled traffic. However, this was still dependent on the flight crew to provide altitude information. As traffic densities increased, controllers were assigned responsibilities for blocks of airspace, including minimum altitudes within those blocks, which were not necessarily known to flight crews while being controlled. The combination of vectoring airplanes on specific headings, and maintaining minimum altitudes within blocks of airspace, provided for safe margins for terrain separation and enhanced the flow of traffic within the airspace block. The addition of automatic altitude and ground speed reporting has further enhanced a controller's capability to direct traffic within an airspace block and maintain a high flow of traffic.
The NTSB commented that with this evolution in capability, and subsequent increases in traffic flow in terminal areas, it has become necessary to direct flights away from published routes, and to clear flights below minimum published altitudes. Flight crews have become more dependent on an air traffic controller to control a flight's altitudes, headings, and speeds while operating in a terminal area. This has resulted in a lessened capability for flight crews to know the terrain over which they are flying, and in some cases has limited a flight crew's knowledge of aircraft position relative to the airport and any obstacles that potentially obstruct the flight path.

The NTSB also noted that disparities in controller and flight crew terminology may result in an inadequate understanding on the part of either the flight crew or controller as to how the airplane is moving through three-dimensional airspace.
Applicable to this accident, the NTSB stated that it was clearly the flight crew's expectation that the controller would have issued an approach clearance that included an altitude restriction, if necessary, for terrain clearance. The flight crew further believed that the flight was under continuous radar surveillance, when, in fact, once having cleared the flight for the approach, the controller no longer monitored the flight. The controller did not consider the flight to be a "radar arrival," as it had not been vectored to the final approach course. The flight was considered by the controller to be operating on its own navigation, and subsequently responsible for its own terrain clearance.
In evaluating the requirements of FAA Handbook 7110.8C, paragraph 1360, the NTSB agreed that the flight was not a radar arrival, but should have been handled as one. The NTSB further stated that the ATC system should have provided for redundancies that would have identified and corrected deviations from a clearance which was not being followed as a controller expected. In the view of the NTSB, the controller should have provided specific information to the flight crew regarding their aircraft's position relative to the approach fix, and a minimum altitude to which the flight could descend prior to reaching the specified approach fix. The NTSB concluded that in this respect, the issued clearance was inadequate, and that its issuance and acceptance by the flight was the result of a misunderstanding between the pilot and controller.

The NTSB also noted a discrepancy in the approach plate that could have misled the crew into descending to too low an altitude. Airports typically have at least one, and may have several different approaches, or types of approaches, to each available runway. Flight 514 was making a non-precision VOR/DME approach to runway 12. An approach plate depicts the local area around an airport (perhaps as far as 20 to 30 miles from the airport), and provides both an overhead and profile view in order to guide a flight onto the proper headings and further provide minimum safe altitudes at specific distances from the airport. For this specific VOR/DME approach, the overhead view on the approach plate provided various intercept headings from which the flight could intercept and maintain the proper VOR radial for final approach to the runway, and noted key landmarks and terrain features that could provide obstacles to the flight path. For the sector from which this approach was being conducted, 3,300 feet was indicated as the minimum safe altitude. Directly along the flight path, 3,400 feet was indicated as the minimum intercept altitude for the final approach heading, and 1,800 feet was indicated at the 12-mile point, along the final approach track. View the original approach plate, employed by Flight 514.
On the profile view, nothing was indicated outside of the six-mile point (19 miles closer to the runway than Mt. Weather), and at the six-mile point, 1,800 feet was indicated as the minimum safe altitude. There was no requirement that the overhead and profile views depict the same information, or to the same ranges from the airport. Coupled with the apparent confusion on the flight deck about minimum safe altitudes, the NTSB commented that the approach plate did not adequately specify the minimum safe altitude for the approach, and could have misled the crew into believing that 1,800 feet was a safe altitude while still 40 miles from the airport. This may have aided the crew in their decision to begin their descent to 1,800 feet, reaching that altitude in a portion of the approach where 3,400 feet was actually the specified minimum safe altitude. In years subsequent to this accident, but in part due to this accident, approach chart formats were changed to be clearer as to minimum safe altitudes. View a copy of the revised approach plate for this approach (revised after the accident).
Ground Proximity Warning System (GPWS)


Photo copyright Paul Robinson - used with permission
At the time of this accident, the majority of commercial aircraft were not equipped with GPWS, and had no consistently positive means to avoid controlled flight into terrain (CFIT) when terrain could not be acquired visually. During this time period, CFIT accidents were prevalent and were the dominant causal factor in transport accidents. GPWS had been developed to mitigate the possibility of CFIT accidents when airplanes were maneuvering close to the ground, or where flight path obstacles may exist, even in low altitude cruise. Flight in inclement weather or at night can increase the risk of CFIT, and GPWS was intended to provide a means to avoid terrain when visual means are not available and ground impact is imminent. GPWS receives its signal from the radio altimeter, and determines whether or not the radio altitude is decreasing, and at what rate. If the terrain closure rate exceeds a threshold level, a voice warning is activated, indicating to the flight crew that evasive action is necessary in order to avert terrain collision. A video describing this feature of GPWS is available below:
The GPWS systems available at the time provided a number of different warning modes. Depending on the phase of flight and terrain closure condition, the GPWS could warn the crew of an excessive descent rate, an excessive terrain closure rate (as occurred in this accident), a descent after takeoff, not being in a landing configuration at too low an altitude, and being below the glide slope during approach. The GPWS system also provided various optional altitude callouts during an approach, and, in newer versions of GPWS, also provides windshear alerting if windshear conditions are encountered.
GPWS has continued to evolve, and modern installations now utilize Satellite (Global Positioning System - GPS) positioning and a worldwide terrain database to determine if obstacles exist in the flight path. Modern systems, referred to as Terrain Awareness Warning Systems (TAWS), operate predictively, in a "look-ahead" mode to provide terrain awareness, alerts, and warnings to the flight crew. The incorporation of these enhanced features further mitigates the hazard of controlled flight into terrain.

Conclusion
In their overall conclusion, the NTSB cited the crew's decision to descend to 1,800 feet, in an area where 1,800 was below the minimum safe altitude, as the primary cause of the accident. However, they also cited a number of contributing factors, which in years following the accident were acted upon by the FAA and industry to mitigate the occurrence of similar accidents. Of the several actions resulting from this accident, the most significant was the requirement to incorporate GPWS into the transport fleet.
Acknowledgement
Mr. C. Donald Bateman is credited with developing the Ground Proximity Warning System (GPWS), one of the most important technologies in commercial aviation. Mr. Bateman was a corporate fellow, and chief engineer at Honeywell’s Aerospace facility in Redmond, Washington where he was the developer of GPWS, and later the Enhanced Ground Proximity Warning System (EGPWS). Both systems have had a major effect on controlled flight into terrain (CFIT) accidents, helping reduce the rate from one in every three million flights to less than one in every 20 million flights. President Barack Obama presented Mr. Bateman with the 2010 U.S. Presidential Medal of Technology and Innovation for his many achievements in advancing commercial aviation safety, including his pioneering work on GPWS in the 1970’s.
The NTSB released 24 findings and issued a probable cause statement. The findings ranged in scope from crew qualifications and flight deck procedures to ATC procedures and the approach procedures documents used on the flight deck. The complete text of the findings is available at the following link: NTSB findings.
The probable cause cited by the NTSB was as follows:
"The National Transportation Safety Board determines that the probable cause of the accident was the crew's decision to descend to 1,800 feet before the aircraft had reached the approach segment where that minimum altitude applied. The crew's decision to descend was the result of inadequacies and lack of clarity in the air traffic control procedures which led to a misunderstanding on the part of the pilots and of the controllers regarding each other's responsibilities during operations in terminal areas under instrument meteorological conditions. Nevertheless, the examination of the plan view of the approach chart should have disclosed to the captain that a minimum altitude of 1,800 feet was not a safe altitude.
Contributing factors were:
- The failure of the FAA to take timely action to resolve the confusion and misinterpretation of air traffic terminology although the Agency had been aware of the problem for several years;
- The issuance of the approach clearance when the flight was 44 miles from the airport on an unpublished route without clearly defined minimum altitudes; and
- Inadequate depiction of altitude restrictions on the profile view of the approach chart for the VOR/DME approach to runway 12 at Dulles International Airport.
The complete accident report can be viewed at the following link: NTSB Accident Report
The NTSB issued 14 recommendations relative to this accident, which are contained in Appendix 1 to the accident report. The complete text of the recommendations is reproduced at the following link: NTSB recommendations
As a result of these recommendations, and subsequent to the accident, the FAA took several actions in an effort to prevent a recurrence of this type of accident.
- The FAA directed that all air carrier aircraft be equipped with a ground proximity warning system by December 1975.
- The FAA revised the provisions of 14 CFR 91 with regard to pilot responsibilities and actions after receiving a clearance for a non-precision approach.
- The FAA established an incident reporting system which is intended to identify unsafe operating conditions in order that they can be corrected before an accident occurs.
- The FAA changed its air traffic control procedures to provide for the issuance of altitude restrictions during non-precision instrument approaches.
- The FAA installed a modification to the ARTS III system to alert air traffic controllers when aircraft deviate from predetermined altitudes while operating in the terminal area.
14 CFR 91.3 - Responsibility and authority of the pilot in command
14 CFR 91.119 - Minimum safe altitudes: General
14 CFR 121.133 - Manual requirements: Preparation
14 CFR 121.135 - Manual contents
14 CFR 121.533 - Responsibility for operational control: Domestic operations
14 CFR 121.567 - Instrument approach procedures and IFR landing minimums
14 CFR 121.657 - Flight altitude rules
14 CFR 121.659 - Initial approach altitude: Domestic and supplemental operations and commercial operators
Testimony at the public hearing for this accident indicated that air traffic controllers may vector flights to various points within an approach area to better position the flight for execution of the approach. Aircraft may be vectored off of published routes, and may also be cleared to altitudes below published minimum altitudes on approach charts. Controllers and pilots have access to the same information regarding minimum altitudes within 25 miles of an airport, and minimum altitudes for various segments of an instrument approach. However, a controller also has available minimum vectoring altitudes which may be used to clear aircraft to altitudes in certain sectors even when those altitudes are below the minimum altitudes on the approach charts. Flight crews have no way of knowing the minimum vectoring altitudes except through experience flying specific approaches. At the public hearing, pilots testified that they had become accustomed to this type of service and frequently might not be aware of their exact location in relation to terrain and obstacles on their approach charts.
Pilot testimony further indicated that flight crews had become so accustomed to controller assistance that, unless advised by a controller, they might not be aware of the type of services they were, or were not, receiving. Witnesses from the FAA testified that it was not necessary for flight crews to know what services they were receiving, as the flight crews bore the ultimate responsibility for maintaining terrain clearance. In the case of TWA 514, the flight was inbound by means of its own navigation, and though it was in a radar environment, it was not considered to be conducting a radar approach. Since it was a non radar arrival, the only controller responsibility was to maintain traffic separation. Once the approach clearance had been issued, it was expected by the controller that the flight would maintain terrain clearance. Further, since they were already established on the inbound approach course, the controller expected that the approach would be completed using the designated approach aids. Also, since the flight was already established on the final approach course, the clearance could be, and was, issued prior to reaching the approach fix.
The flight, on the other hand, was expecting that if a minimum safe altitude was applicable, they would have been notified when receiving the approach clearance. The fact that the approach plate did not provide a depiction of required flight paths or prominent specifications of minimum safe altitudes beyond six nautical miles from the runway further confused the crew. This combination of factors misled the crew into believing that it was safe to descend to 1,800 feet while still more than 40 nautical miles from the airport.
Descent to final approach fix altitude at a distance from the airport where terrain and obstacles extended to the same altitude -
- The approach procedure specified that until the flight reached a point 18 nmi from the airport, the minimum safe altitude was 3,400 feet, reducing to 1,800 feet six nmi from the airport. Flight 514 began descending when at a distance of 44 miles from the airport, and according to the NTSB accident report, reached 1,800 feet just before impacting Mt. Weather, about 25 miles from the airport. The approach was being conducted in instrument meteorological conditions and turbulence, in a designated mountainous area, and visual contact with the ground was intermittent. The investigation concluded that the captain did not know his exact position relative to the airport and was not aware of the flight's low altitude relative to the surrounding terrain.
Issuance of an approach clearance without an altitude restriction prior to reaching the final approach fix -
- When Flight 514 was 44 miles from the airport at an altitude of 7,000 feet, the air traffic controller cleared the flight for the approach but did not issue an accompanying altitude restriction. Following receipt of the clearance, the flight descended to 1,800 feet, reaching that altitude 25 nmi from the airport, just prior to impact with Mt. Weather. At that distance the minimum altitude specified should have been no lower than 3,400 feet, according to the associated approach procedure. Had an altitude restriction been issued, the airplane would have been at a higher altitude until reaching the final approach fix and would have passed above Mt. Weather.
Lack of a ground proximity warning system to provide terrain awareness during the approach -
- Flight 514 descended below a minimum safe altitude early in the approach. The approach was being made in inclement weather, and ground visual contact was intermittent. As a result, the flight crew was not aware that they were at a very low altitude with respect to the local terrain until the radio altimeter provided an aural alert that they had descended below a previously set threshold altitude above the ground. The alert did not, in this case, provide a sufficiently timely warning to allow terrain avoidance. Following the accident, installation of ground proximity warning systems was mandated on the commercial fleet. The NTSB stated that if a GPWS-like system had been installed on flight 514, the accident would have been averted.
The flight crew assumed that when cleared for the approach, independent of their distance from the airport, they could safely descend to the final approach altitude, and further, that they would continue to be under radar surveillance.
Safety would be achieved, and CFIT accidents would be avoided by adherence to published approach procedures and information, and air traffic control procedures.
During the course of the investigation of TWA Flight 514, it was learned by the NTSB that in October 1974 a United Airlines flight, flying the same approach, had a CFIT near-miss event similar to TWA 514, but it did not report the event outside the carrier's own system. During initial phases of the approach, and established at 6,500 feet, the UAL flight was issued a clearance to 4,000 feet and instructed to contact Dulles approach control. The flight was cleared for a VOR approach to runway 12. Following the clearance, the flight descended to 1,800 feet and intercepted the 300-degree radial (120 degrees inbound) to the Dulles VOR and landed without incident.
After landing, the crew reviewed the approach and concluded that they had descended to 1,800 feet about 25 nmi from the VOR. They reported that at the time the approach clearance was received, they had believed they were cleared to descend immediately to the final approach altitude, rather than wait until they were six miles from the airport, which was specified on the approach plate as the point at which 1,800 feet was authorized.
The carrier investigated the incident, including contact with FAA at the Dulles traffic control tower. It was agreed that in the future, a clearance for this approach would be issued when the airplane was about 30 nmi from the airport, and that future flights would be radar monitored unless higher priority activities and duties precluded radar monitoring.
As a result of this internal investigation, the carrier concluded that it was not necessary to contact the FAA, to submit any recommendations to the FAA, or to change procedures. The carrier did publish an internal notice to all flight crews, as follows:
"The extensive use of radar vectoring, in terminal areas, has led to some misunderstanding on the part of flight crews.
Recent.......events prompt these reminders:
- The words 'cleared for the approach' generally put the flight crew on their own.
- Don't start down to final approach fix altitude without reviewing other altitude minimums.
- Inbound minimum altitudes to outer fixes are on the Jepp plates.
- Flight crews should thoroughly familiarize themselves with the altitude information shown on approach and/or area charts for the terminals into which they are operating. This includes minimum segment altitude (MSA) information."
Following this event, had this information been more widely distributed (i.e., outside the affected carrier), or the FAA been contacted regarding the carrier's findings, the TWA 514 accident might have been avoided.
As a result of this event, and other operational events occurring fleet wide, the Aviation Safety Reporting System (ASRS) was developed as a means to voluntarily report operational errors. Reports submitted to ASRS may not be used in enforcement actions by the FAA. The reporting system is currently maintained by the National Aeronautics and Space Administration (NASA) ASRS can be accessed at: http://asrs.arc.nasa.gov/
Following this accident, the FAA initiated:
- A fleet-wide requirement for installation of Ground Proximity Warning Systems in all air carrier aircraft by December 1975
- Revisions to 14 CFR part 91 with regard to pilot responsibilities and actions after receiving a clearance for a non-precision approach
- Creation of the Aviation Safety Reporting System, managed by NASA
- With regard to terrain clearance, subsequent CFIT-type accidents have led to an evolution of GPWS capabilities, resulting in enhanced GPWS (TAWS) systems
- Issuance of rulemaking by the FAA in 2002 that made the installation of TAWS mandatory throughout the air carrier fleet
- Modification of air traffic control procedures such that altitude restrictions are issued during non-precision instrument approaches
- Installation of a modification to the ARTS III altitude reporting system such that controllers receive alerts when a flight deviates from predetermined altitudes when operating inside a terminal area.
This accident was attributed to errors and misunderstandings on the part of the flight crew and had contributing factors related to air traffic control procedures and pilot and air traffic control responsibilities. The airplane was functioning as intended. As a result, no airworthiness directives were issued related to this accident.
Installation of GPWS was made mandatory by a retroactive application of the affected operating rules, and as a result, AD's to require GPWS installations were not issued.
Airplane Life Cycle:
- Operational
Accident Threat Categories:
- Crew Resource Management
- Incorrect Piloting Technique
Groupings:
- Controlled Flight Into Terrain
- Approach and Landing
Accident Common Themes:
- Organizational Lapses
- Human Error
Organizational Lapses
The approach plates used by the flight crew contained information regarding both profile and overhead (heading) information required to conduct the approach. However, at the time of this accident, the profile view only extended to six nautical miles from the airport, while the overhead information extended to more than 30 miles. The profile view required an altitude of 1,800 feet at the final approach fix, and the overhead view specified an altitude of 3,400 feet at the initial approach fix, at a distance of approximately 18 miles from the airport. The discrepancy in the two views was not immediately noticeable and led to confusion in the flight deck, eventually leading to the crew's decision to descend to 1,800 feet. As a result of this accident, approach procedures were modified such that altitude restrictions were issued by controllers when clearing a flight for a non-precision approach, and altitude alerts are now provided to controllers when a flight deviates from a predetermined minimum altitude during an approach.
Human Error
Flight 514 was conducting an approach that was unfamiliar to the crew and was the result of having to divert from the intended destination airport. As a result of confusion over information published on the approach plate, the crew of Flight 514 determined that once cleared for the approach, the flight was allowed to descend to 1,800 feet, the altitude specified for the initial approach fix. At the time of initiation of descent, the flight was still 40 miles from the airport. The crew discussed other information on the approach plate that specified 3,400 feet as a minimum altitude until much closer to the airport, but eventually agreed that since they had been cleared for the approach, all other altitude restrictions were removed, and 1,800 feet was an allowable descent altitude. In fact, 3,400 feet was the correct minimum altitude until reaching a point approximately 18 miles from the airport. As a result of descending to 1,800 feet and arriving at that altitude while still further than 25 miles from the airport, the airplane hit the western slopes of Mt. Weather at approximately 1,800 feet.
Alaska Airlines B-727, Juneau, Alaska, September 4, 1971
Alaska Airlines Flight 1866, a Boeing 727, crashed during approach to Juneau, Alaska. The flight was attempting a non-precision instrument approach to Runway 8, and had reported passing the final approach fix inbound to the airport. No further communications were heard from the flight.
The airplane struck a slope in the Chilkat Mountain range at about the 2500 foot level, approximately on the correct inbound course and 18.5 miles west of the airport. All 104 passengers and seven crewmembers were killed, and the aircraft was destroyed.
The NTSB determined that the probable cause of this accident was a display of misleading navigational information concerning the flight's progress along the localizer course which resulted in a premature descent below obstacle clearance altitude. The origin or nature of the misleading navigational information could not be determined.
The Board further concluded that the crew did not use all available navigational aids to check the flight's progress along the localizer nor were these aids required to be used. The crew also did not perform the required audio identification of the pertinent navigational facilities.
A copy of the NTSB accident report is available here: (Juneau Accident Report)
Air Inter A320, Strasbourg, France, January 20, 1992
While approaching an airport surrounded by mountainous terrain at night, the crew of the Air Inter A320 was offered, and accepted, a change in runway to expedite their arrival at the gate.
In the aftermath of rapidly reprogramming the flight deck automation during a high workload phase of flight, the airplane impacted terrain 10.5 miles from the runway. Eighty-two passengers and five crew members died in the accident. The probable cause of the accident was attributed to the flight crew having inadvertently selected the vertical speed (VS) mode rather than flight path angle (FPA) and mistakenly input a vertical speed of 3,300 feet per minute rather than an FPA of 3.3 degrees during the final segment of the approach.
Among the contributing factors were:
- Autopilot mode confusion on the part of the crew
- Crew input error to the autoflight system
- Improper mode selection (VS verses FPA) or improper mode value (3.3 verses 3,300) input
- Lack of awareness of the airplane's vertical speed on the part of the flight crew
- Lack of the crew's adherence to established instrument approach procedures in performing checks of the altitude, distances, and aircraft automation
- Lack of communication on the part of the crew
- Improper use of crew resource management (CRM)
- Design of the autoflight system controls and the resultant potential for mode confusion and input errors
- Late change of instrument approach selection
- High crew workload resulting from the change of approach procedure late in the terminal phase of the flight
- GPWS was inoperative
See accident module
American Airlines B-757, Cali, Colombia, December 20, 1995
On the evening of December 20, 1995, at approximately 2142 Eastern Standard Time (equivalent to Cali, Colombia local time), American Airlines Flight 965 crashed into high terrain during approach to Alfonso Bonilla Aragon International Airport, Cali, Colombia. Of the 163 people on board only four survived. The weather conditions that night were relatively clear skies and light surface winds with no moon.
The airplane involved in this accident, a Boeing 757, was equipped with cathode ray tubes (CRT), or "glass cockpit" technology, including screens which display flight path and navigation information, engine information, and a Flight Management System (FMS). A GPWS was also installed and functioned normally at the time of the accident.
The investigation concluded that this accident was attributed to flight crew human error involving navigational and crew resource management lapses. This CFIT accident became the catalyst for requiring the installation of TAWS in transport airplanes.
See accident module
Technical Related Lessons
Instrument approach procedures, including radio communication terminology between airplane and air traffic controllers, must be clear and unambiguous, and should include altitude restrictions if necessary to avoid terrain or flight path obstacles. (Threat Category: Incorrect Piloting Technique)
- As stated in the accident report, and during the public hearings related to this accident, Flight 514 was "cleared for the approach" while still 44 nautical miles from Dulles International Airport. No altitude restrictions were issued by the air traffic controller, and the flight crew interpreted the onboard printed approach information as allowing a descent to a minimum altitude of 1,800 feet. In fact, for the initial segment of the approach, the minimum published altitude was 3,400 feet, until reaching a navigational intersection that was approximately 18 miles from the airport and after passage of Mt. Weather. The lack of an altitude restriction from the controller, in combination with errors on the approach plate, along with confusion among the flight crew about the minimum allowable altitude, were all cited as contributing factors in this accident.
Controlled flight into terrain (CFIT) presents an operational problem that requires a multi-pronged solution to provide a consistently acceptable level of safety. Safety strategies should include GPWS, clear, unambiguous approach publications, standardized approach procedures, and standardized communication procedures between controllers and aircraft, (Threat Category: Incorrect Piloting Technique)
- The NTSB cited a number of deficiencies during the approach that resulted in the accident. Poor communication, lack of flight deck equipment, and deficiencies in the approach plates all contributed to the early descent and eventual flight into terrain. Since the accident, GPWS has been mandated, and has evolved into a more sophisticated terrain avoidance system (TAWS), which is predictive in nature, and communication and flight procedures have become more standardized. While CFIT accidents do still occur, their incidence has been greatly reduced by the advances in all the stated areas.
Common Theme Related Lessons
Safety critical flight or procedural information must be provided to flight crews in easily understandable formats and language in order to avoid confusion or mistakes in execution (Common Theme: Organizational Lapses)
- The NTSB cited deficiencies on the approach plate as a factor in this accident. While the overhead view indicated that the minimum safe altitude for the initial approach segment should have been 3,400 feet, the profile view did not extend to the same range from the airport, and at the six nautical mile range point that was indicated, specified an altitude of 1,800 feet. This discrepancy was not immediately noticeable and led to confusion on the flight deck as to the correct descent altitude, and the eventual decision to descend to 1,800 feet rather than 3,400 feet.
Deviations from customary, or "normal" operational situations, can increase the risk for subsequent human error. When flight crews encounter these non-routine situations, rigorous adherence and vigilance to training and procedures are particularly critical. (Common Theme: Human Error)
- TWA Flight 514 was originally bound for Washington National Airport. After becoming airborne, the crew learned that inclement weather had forced the closure of Washington National Airport, and a diversion to Dulles was required. With the unexpected and unplanned diversion, the crew was required to become familiar with the approach procedures for Dulles and execute an approach which they had not originally planned, and in a limited amount of time in inclement weather.