
Airbus A320-111

Photo copyright Pedro Aragao - used with permission
Air Inter, call sign ITF 148 DA, F-GGED
Strasbourg, France
January 20, 1992
Air Inter, call sign ITF148 DA, was on a scheduled night flight between Lyon and Strasbourg, France. The flight departed Lyon at 1740 local time. The crew originally planned to fly an approach to runway 23 at Strasbourg. However, runway 05 was the active runway and the crew, after being advised that an approach to runway 23 would create delays, accepted the approach to runway 05. At that time, the airplane was very close to the point where the approach would begin. During the initial phases of the approach, while maneuvering to align with the runway, the flight began a very steep descent, after which no further transmissions were heard from the aircraft. The aircraft impacted La Bloss Mountain at an elevation of 2,620 ft, 0.8 nautical miles (nm) left of the final approach course and 10.5 nm from the end of the runway. Eighty-two passengers and five crew members died in the accident.
The Commission of Investigation determined that the cause of the accident was the development of an unusually high descent rate that was not corrected by the crew. The investigation retained two hypotheses regarding the cause of the descent:
- (Quite probable) misunderstanding involving vertical mode (resulting either from an omission to change the trajectory reference, or from poor execution of the command to change it) or of an error in displaying the consigned value (mechanical digital display of the numeric value given out during the briefing).
- (Very improbable) hypothesis of a malfunction of the Flight Control Unit (FCU) (fault in the push-button used for changing mode, or corruption of the consigned value, displayed by the pilot on the FCU before it is captured by the Autopilot computer).

Photo copyright Andy Pope - used with permission
History of the Flight
On January 20, 1992, an Airbus A320 airplane registered F-GGED and operated by Air Inter was on a scheduled night flight between Lyon-Satolas airport (now called Lyon-Saint Exupery) and Strasbourg-Entzheim airport, both in France. The flight departed Lyon at 1720 local time with 90 passengers and six crewmembers aboard. The flight was uneventful en route to Strasbourg. The captain in the left seat was the pilot flying (PF), and the first officer in the right seat was the pilot not flying (PNF).
The airplane's autopilot and autothrottle were engaged during the entire approach phase. The Automatic Terminal Information Service (ATIS), which gives the flight crew a description of weather conditions and runway status, reported winds of 30 knots and layers of scattered to broken clouds at 1,100 and 2,600 feet above the ground.
Although ATIS announced that the active runway was 05, the flight crew discussed the winds and weather conditions and planned to fly an Instrument Landing System (ILS) approach to runway 23 at Strasbourg, followed by a visual landing on runway 05. At 1809 local time, upon entering the terminal area for Strasbourg, the flight was cleared by the Approach Air Traffic Controller (ATC) to descend to 5,000 ft. The airplane was approximately 25 nm southwest of its destination at this point, and approximately 12 nm from intersection ANDLO, part of the approach procedure for the VOR DME runway 05 approach.
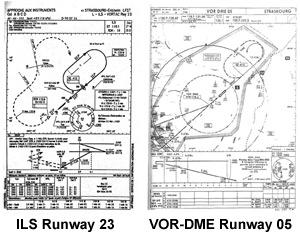
View ILS Runway 23
View VOR DME Runway 05
After the airplane passed ANDLO intersection, the approach air traffic controller cleared the flight for the VOR-DME approach to runway 05. At that time, the airplane was almost over the Strasbourg VOR (STR), approximately 2 ½ nm to the southwest of the airport. The flight crew made a request to the controller to fly the ILS to runway 23, followed by a visual approach to runway 05. The controller responded by informing the crew that this would result in a delay, as there were three aircraft waiting to take off from runway 05. The flight crew then agreed to accept the complete VOR-DME 05 approach. The approach controller suggested radar guidance to bring the airplane back towards ANDLO intersection in order to shorten the approach procedure, and the flight crew accepted. At this point the aircraft was essentially over the Strasbourg VOR and still descending towards its assigned altitude of 5,000 ft. The controller issued instructions to turn left to a heading of 230 degrees magnetic, putting the airplane on an outbound track parallel to the VOR DME runway 05 inbound final approach course. Shortly after beginning this left-hand turn, the airplane was leveled at 5,000 feet.

While proceeding on the outbound track, the captain, adjusting from the planned approach to runway 23 to the assigned approach to runway 05, briefed elements of the approach procedure, including the glide path angle, which the captain noted was equivalent to 3.3 degrees. At 1818 local time, air traffic control (ATC) issued a left turn to a heading of 090 degrees and the captain used the autopilot's heading mode to comply with the ATC vectors. This would set the airplane up towards intercepting the final approach course, inbound to the airport. Approximately 35 seconds later, the airplane's flaps were selected to "Flaps 1." After 20 more seconds had elapsed, ATC issued a further left turn to 051 degrees, but noted that the airplane was "askew" to the left of ANDLO intersection. The first officer, seeing that the airplane would not be overflying ANDLO as expected, commented to the captain that "we're going inside," and suggested a small turn back to the right (to a heading of 070) to intercept the final approach course.
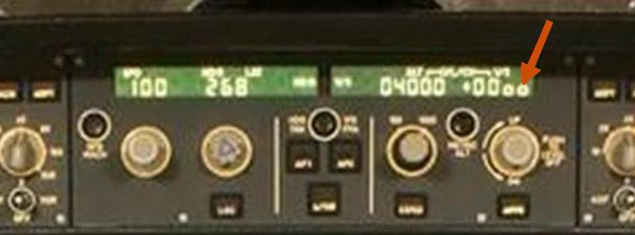
At 1819, still under the control of ATC and level at 5,000 ft, the flight was cleared for final approach. Shortly thereafter the flaps were selected to "Flaps 2," the landing gear was lowered, and approximately at a position allowed by the approach procedure, the aircraft initiated its descent. As the descent began, the controller instructed the flight crew to report when the airplane was over the VOR, and the flight crew acknowledged. The acknowledgment was the last transmission from the flight. The flight began its descent 11 nm from the Strasbourg VOR. The investigation concluded that, based on conversation on the cockpit voice recorder, the descent was intended to be performed at a normal negative 3.3 degrees flight path angle. However, the investigators noted that the actual commanded descent was 3,300 ft/min, and while not conclusively established, may have been the result of inadvertently selecting the vertical speed mode. In this case, "-33" would have appeared on the autopilot display, implying 3,300 ft/min descent, while in the flight path angle mode, "-3.3" would have appeared in the same window.

Approximately 30 seconds after beginning the descent of 3,300 ft/min and at 1,000 feet above the local terrain, the captain, who was flying the approach, remarked, "need to watch...descent." Virtually simultaneously, the first officer noted that the airplane was almost on the final approach course. Fifteen seconds later, with the airplane still in a rapid descent, the radar altimeter aural announced, "TWO HUNDRED," indicating that the airplane was 200 feet from the ground. Approximately 45 seconds after having initiated the descent, the airplane struck the ground.

The wreckage was found at 2235 local time on La Bloss Mountain at an elevation of 2,620 ft, 0.8 nm left of the final approach course and 10.5 nm from the end of the runway. Eighty-two passengers and five crew members died in the accident. The aircraft was completely destroyed.
A320 Flight Deck and Flight Control Unit--Display and Function
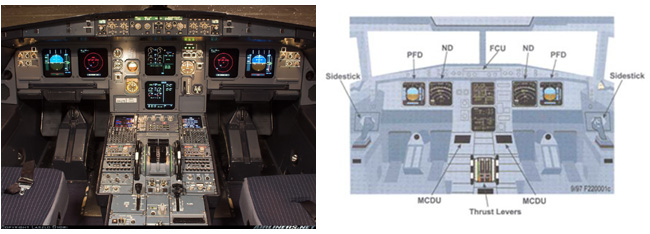
The A320 cockpit is equipped with a number of displays. The Primary Flight Display (PFD) depicts aircraft flight parameters such as attitude, airspeed, and altitude, while the Navigation Display (ND) displays navigational information. The A320 is equipped with an autopilot, which responds to pilot input via the Flight Control Unit (FCU) mounted centrally on the flight deck glare shield.
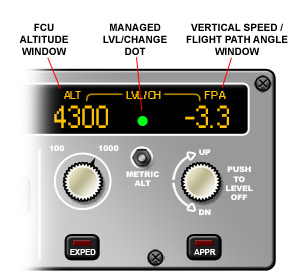
Selection Panel
The autopilot system allows for control of the lateral path (through control of heading or lateral navigation path) and, germane to the Air Inter accident, the vertical path. Vertical path control includes the vertical speed, or "VS" mode, whereby the autopilot responds to pilot input of a desired vertical speed in units of feet per minute climb or descent, and the flight path angle, or "FPA" mode, in which the pilot inputs the desired flight path angle in degrees. Control and display of VS or FPA commands are made via the FCU. These two modes share a common location for pilot control of VS or FPA as well as display of selected input. A pushbutton toggles the selected mode between VS and FPA. Rotating the toggle pushbutton allows selection of the target VS or FPA.

At the time of the accident, the displays for the two modes were very similar. Vertical speed was indicated by two digits representing the VS in hundreds of feet per minute, and FPA was indicated by two digits, separated by a decimal point. Investigators concluded that in the minutes preceding the accident, while configuring the airplane for approach, the flight crew may have intended to select a -3.3-degree flight path angle (which would have been depicted as "-3.3") but may have inadvertently selected a vertical speed of -3300 feet/min (which would have been indicated as "-33"). The active mode (VS or FPA) would also have been annunciated near the numerical indications. The investigation did not establish conclusively that the flight crew made this error but did state that it was highly probable.
Subsequent to the accident, the displays were updated such that if vertical speed were the selected mode, two additional zeros would be displayed. Thus, a VS of -3300 ft/min would be displayed as "-3300". In addition to control of VS and FPA via the FCU, the PFD displays the modes selected and specific VS rate or FPA angle. An animation of the flight path during the final minutes of the flight, and a comparison of the flight path effects of the two autopilot modes, is available below.
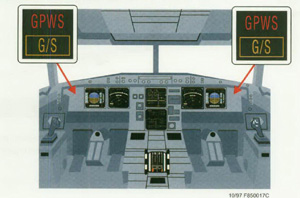
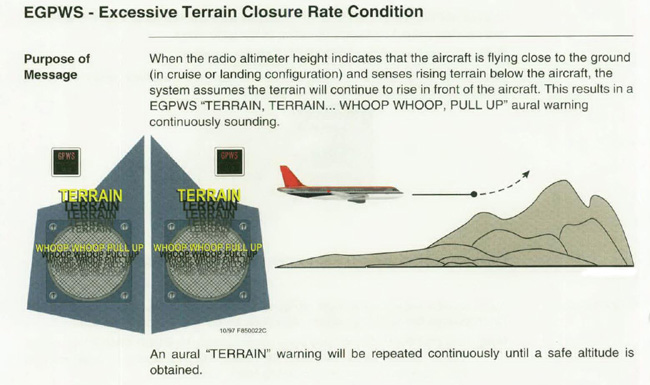
Ground Proximity Warning Systems (GPWS)
Ground Proximity Warning Systems (GPWS) are designed to reduce the risk of controlled flight into terrain (CFIT) accidents. A GPWS alerts a crew to impending collision with terrain by using a variety of available on-board information such as position, speed, and radio altimeter height above the ground. Both visual and aural alerts are provided to the flight crew. In 1975, after a December 1974 Boeing 727 accident near Dulles Airport, Washington D.C., FAA regulations were modified to require large commercial U.S. registered aircraft to be equipped with GPWS. Despite some initial problems (including erroneous alerts and/or alerts occurring during normal operations where airplane safety was not in jeopardy), studies conducted at the time in the United States indicated a reduction in the number of CFIT accidents had been achieved and was attributable to GPWS. More specifically, over the five years prior to 1975, an average of 2.8 CFIT accidents per year had occurred in the United States. The period during which GPWS was installed in the U.S. transport airplane fleet extended from mid-1974 to the end of 1976. The number of CFIT accidents then fell appreciably: 0 in 1975, 2 in 1976 and 1977, 1 in 1978, and 0 from then on with the exception of 1985 (1) and 1989 (2).
These positive safety results led the International Civil Aviation Organization (ICAO) in 1979 to include among its standards the requirement to equip all turbine-powered aircraft with a maximum takeoff weight exceeding 15,000 kilograms, or authorized to carry more than 30 passengers, with a GPWS. ICAO stipulated that aircraft receiving an Airworthiness Certificate on or after July 1, 1979, be equipped with a GPWS. For those aircraft that had received an Airworthiness Certificate before July 1, 1979, a GPWS was only recommended. According to a study by the GPWS manufacturer at the time of the Air Inter accident, approximately 95% of the world fleet meeting the criteria of aircraft required to carry a GPWS as defined by the ICAO were, in fact, so equipped.
From January 1983 to April 1991, the confidential Aviation Safety Reporting System (ASRS) noted 64 reports of crews which had experienced a GPWS alert. In at least 35 cases, flight crews reported that the GPWS warning had prevented an accident.
The situation in France, as documented in the accident report, with regards to adopting GPWS as a system required by regulation, was different than ICAO at large. The following factors were noted: A test program to evaluate the system had been carried out by the CEV (Centre de Essais en Vol - the French Flight Test Centre) in 1975. Taking into account the level of spurious alarms encountered during this program, the French government concluded that the GPWS afforded safety gains which were less positive than had been indicated by the U.S. studies. A letter from the French government sent to the ICAO in 1977 stated that the carrying of a GPWS should have "at most the status of a recommended practice," and not of a standard. However, the ICAO decided to include the installation of GPWS among its standards. In 1978 ICAO was notified that France would be making an exception concerning GPWS standards.

Following a subsequent inquiry by the ICAO into national variations, as noted in the accident report, France replied, in error, that its regulations did not contain any exceptions and, therefore, the note indicating a French derogation on this point was removed from ICAO documents. In 1990 the European Joint Aviation Authorities (JAA) began the task of developing common European operational regulations. The draft regulations required, beginning March 1, 1993, that GPWS systems be installed. At the time of the Air Inter accident (January 1992), French regulations did not make the installation of a GPWS mandatory. Even so, as of December 31, 1991, approximately 75% of the aircraft operated by French carriers, and meeting the ICAO criteria for carrying a GPWS, were equipped with such a system. Air Inter, based on the results of the CEV tests, elected not to install GPWS systems on its aircraft.

Air Inter company had participated in the CEV trials carried out in November 1975. The trials were conducted on Mercure and A300 aircraft and included flights by Air Inter crews over the company route structure in 1976 and 1977. In view of the fact that a high number of "nuisance", or inappropriate alarms was observed during these evaluations of the initial GPWS versions, and given the absence of any statutory requirement, Air Inter chose not to equip its fleet with GPWS. However, following technical improvements to the GPWS, at the end of the 1970's, Air Inter began procuring equipment to provision their A300 and Mercure aircraft. They had also begun acquiring equipment for the A320 but had not begun installations on their A320 fleet.
Flight Crew Interaction

The accident report devoted significant comment to the personal interaction of the two pilots, and an apparent lack of cooperation, leading to a breakdown in good crew resource management (CRM) practices. The accident report stated that the relationship between the two pilots was subdued, and though not hostile, was strained. Prior to the flight, they had never met nor flown together. The investigation established that there was a "serious lack of communication" between the crew members, based most probably on personality differences, and a "lack of affinity." The result was a breakdown in flight deck protocol and procedures, and a lack of attention to the airplane position and progress of the approach. The investigation established that a number of procedurally required callouts were omitted during the approach, and both crew members focused on the lateral flight path to the detriment of the vertical path monitoring. Standard procedures and crew communication seemed to have completely broken down, leading to a loss of situational awareness and the development of the high descent rate prior to impact. The investigation concluded that if proper flight deck discipline and adequate CRM procedures had been followed, the arrival approach options would have been discussed, and an approach plan agreed upon by the two pilots. Cross-crew communication would have been established and maintained, and the flight path would have been properly monitored, potentially avoiding what appeared to have been an error or oversight in configuring and verifying the vertical flight path.
Human Factors-Federal Aviation Administration Human Factors Team Report on: The Interfaces Between Flight Crews and Modern Fight Deck Systems, dated June 18, 1996
Many accidents have highlighted difficulties in flight crew interactions with flight deck automation. The FAA, along with U.S. and foreign authorities, manufacturers and operators, launched a study to evaluate the flight crew/flight deck automation interfaces of current generation transport category airplanes. This report is a culmination of that study. The purpose of this study was to identify opportunities for improvements which could be applied in future regulatory and policy development associated with flight crew/flight deck automation interfaces. The report can be viewed at the following link: (Human Factors Report)

The Commission of Investigation issued a number of findings on several different aspects of the investigation. The complete text of the various findings is available by accessing the associated link in the list of findings.
The Commission made a number of General Findings related to the circumstances of the accident: airplane airworthiness, crew qualifications, condition of navigational aids, and the flight path of the airplane prior to the crash. Those findings can be accessed here: (General findings)
The Commission also made a number of findings related to specific factors in the accident. These findings can be access by accessing the specific links:
The largest number of findings was related to the direct causes of the accident. Those findings can be accessed here:
The Commission found that the pivotal event in the accident sequence was the development of an abnormally high descent rate that was not corrected by the crew.
The complete English language version of the accident report is available at the following link: (Accident Report)
- Recommendations concerning the crew
- These recommendations deal primarily with aspects of crew training, crew pairing, human factors, and crew resource management.
- Recommendations concerning GPWS
- These recommendations addressed the lack of a requirement for GPWS on French air carrier operators, the incorporation of GPWS into the fleet, and associated crew training objectives.
- Recommendations concerning instruments
- These recommendations addressed onboard and ground-based recording equipment used as part of the accident investigation, including legalities associated with custody of, and access to, various recorded data following an accident.
- Recommendations regarding flight crew interfaces, and autoflight systems
- These recommendations addressed the autoflight system on the A320, crew interface with the system, and aspects of mode and flight path displays.
- Recommendations on survival
- These recommendations addressed various survival aspects of the accident, including post-accident search and rescue.
- Recommendations concerning air traffic control
- These recommendations addressed various air traffic control aspects of the accident.
- Recommendations regarding state supervision
- These recommendations addressed the level of government oversight at Air Inter.
- Recommendations from hindsight
- These two recommendations addressed factors directly related to administrative aspects of the accident investigation.

Joint Aviation Regulations (JAR)
25.771 Pilot Compartment
25.777 Cockpit Controls
25.1303 Flight and navigation instruments
25.1309 Equipment, systems and installations
25.1329 Automatic pilot system
Advisory Circular Joint (ACJ)
25.1329 Automatic Pilot (Interpretative Material and Acceptable Means of Compliance)
JAA Special Condition S30 - Autoflight System
The pertinent portion of this special condition required: "Means must be provided of indicating to the flight crew the active mode and all the modes armed by the pilot. The position of the mode selection button is not an acceptable means of such an indication."
Controlled flight into terrain (CFIT) has been a major cause of accidents in transport aviation. A major U.S. study concluded that between 1979 and 1989, nearly 50% of fatalities in transport aviation were the result of CFIT accidents. Concern over the magnitude of this problem led to the development of early ground proximity warning systems (GPWS).
In 1974, following a TWA 727 accident near Washington, D.C., the FAA required the installation of GPWS on the U.S. air carrier fleet. Following this requirement, the rate of CFIT accidents in the United States dropped markedly. In 1979, in response to this apparent safety improvement, the International Civil Aviation Organization (ICAO) adopted a standard to require installation of GPWS. At the time of the Air Inter A320 accident, approximately 95% of the world's transport fleet was equipped with GPWS. During this same time period, these early versions of GPWS seemed to be experiencing a high rate of false or nuisance GPWS warnings, leading some to question the value of the equipment. As a result, newer versions were developed, and, at least in the United States, air traffic procedures were tailored to the envelope and warning requirements of GPWS.
Beginning in 1975, the French Flight Test Center, initiated a series of GPWS equipment trials. Encountering a high number of incorrect warnings (warnings which occurred when airplane safety was not in jeopardy) the French government concluded that GPWS did not provide the safety gains that had been the basis for U.S. regulatory activity. As a result, the French government adopted the installation of GPWS as a recommended practice, rather than as a regulatory standard. As a consequence, at the time of the accident, though many French air carrier aircraft were equipped with GPWS, it was not a requirement, and Air Inter had not installed GPWS on any of its fleet, including the A320. The accident report, in section 118.2 includes an extensive discussion of the history of GPWS on French carriers.
- High rate of descent on approach, leading to ground impact a distance from the airport
- Lack of a GPWS
- Poor flight crew communication and coordination, leading to a loss of situational awareness
- GPWS was not required to improve ability to avoid CFIT accidents
- The Flight crew would properly monitor the engaged state of the autopilot system, as well as the rate of descent while on final approach to the airport
Controlled flight into terrain accidents have historically been a significant subset of overall accident occurrences. The two CFIT accidents listed here are included elsewhere in this library and were major drivers in the recognition that GPWS would be a contributor in reducing CFIT accidents.
December 29, 1972, Eastern Airlines Flight 401, Lockheed L-1011
While in a holding pattern following an unsafe gear indication on approach to Miami International Airport, the autopilot was inadvertently disconnected while the flight crew performed troubleshooting procedures on the nose landing gear. The airplane began a slow descent that was not detected by the flight crew. As a result, the airplane descended into and crashed in The Everglades. While the circumstances of this accident are somewhat different from those of the Mt. St. Odile accident, it was one of the accidents that indicated a need for a system that could make a flight crew aware of impending ground collision in time to correct the flight path, and thereby avoid an accident.
See accident module
December 1, 1974, TWA Flight 514, Boeing 727
On approach to Dulles International Airport in Washington, D.C., the flight was cleared for a non-precision approach and descended to an unsafe altitude while still 25 miles from the airport. Aligned with the extended centerline of the assigned runway, the flight struck Mt. Weather at an altitude of approximately 1,800 feet. The NTSB determined that the minimum safe altitude in the area of Mt. Weather was 3,400 feet, and that the crew had mistakenly descended to 1,800 feet, with the belief that once cleared for the approach they were cleared to the minimum altitude of 1,800 feet depicted on the approach plate. The accident airplane was not equipped with GPWS, and as a result of this accident, the FAA mandated the installation of GPWS on all commercial flights. The accident further resulted in revisions to the associated approach plate to more clearly depict the minimum safe altitudes and changes to air traffic procedures regarding non-precision approaches.
See accident module
At the time of the accident, GPWS was not required to be installed on the French airline fleet. Following the accident, with the inception of the Joint Aviation Authorities (JAA) JAR-Ops requirements, JAR-OPS 1.665, Ground Proximity Warning Requirements, was adopted. This regulation required the installation of a GPWS on certain (essentially all) transport airplanes operating under JAA requirements.
14 CFR 25.1329 Flight Guidance System
In April 2006, the referenced rule to include specific requirements regarding minimization of flight crew errors and confusion concerning the behavior and operation of the flight guidance system. Further, the FAA updated Advisory Circular AC 25.1329-1B, which includes a large amount of material regarding flight deck indications and alerts, engagement of the flight guidance system, and how the human-machine interface should be designed and evaluated. Both the rule and the AC were intended to directly address many of the findings of the Commission of Investigation on this accident.
The European Aviation Safety Agency (EASA) also adopted similar requirements and guidance material as a result of harmonization activity.
Though Airbus revised the design of the autopilot interface, no airworthiness directives were issued as a result of this accident.
Airplane Life Cycle:
- Operational
Accident Threat Categories:
- Crew Resource Management
- Flight Deck Layout / Avionics Confusion
- Incorrect Piloting Technique
Groupings:
- Controlled Flight Into Terrain
- Automation
- Approach and Landing
Accident Common Themes:
- Organizational Lapses
- Human Error
Organizational Lapses
As addressed in the accident report, the aviation industry, beginning in approximately 1975, had required installation of GPWS in the air carrier fleet in many countries worldwide. As a result of independent studies, the French government had concluded that GPWS did not provide a safety benefit sufficient to require the installation on French air carrier aircraft. The French government recommended installation but did not require it. Therefore, the Air Inter fleet was not equipped with GPWS. The accident report concluded that if GPWS had been installed, the accident would most likely have been avoided.
Human Error
During the latter stages of the approach, the Commission of Investigation concluded that an incorrect autopilot mode was engaged, the result of either a flight crew error, or a failure in the autopilot itself. In either case, the investigation concluded that the flight crew did not correct the error. The engaged autopilot mode produced an excessive descent rate, leading to collision with terrain some distance from the airport. The investigation further stated that the mode display on the autopilot control panel was sufficiently ambiguous that a flight crew, during a high workload flight phase, might fail to recognize the mode that had been selected, or have difficulty distinguishing between the modes, given that both modes were controlled by the same switch (with alternating pushes on the switch toggling between the two different modes of engagement), and the associated mode displays were very similar, making mode identification difficult. Following the accident, the autopilot control panel was modified to simplify autopilot mode identification.
December 29, 1972, Eastern Airlines Flight 401, Lockheed L-1011
While in a holding pattern following an unsafe gear indication on approach to Miami International Airport, the autopilot was inadvertently disconnected while the flight crew performed troubleshooting procedures on the nose landing gear. The airplane began a slow descent that was not detected by the flight crew. As a result, the airplane descended into and crashed in The Everglades. Eastern Airlines Flight 401 was an early accident, indicating the need for some type of system to warn of impending ground collision and allow a flight crew to respond in time to avoid impact.
See accident module
December 1, 1974, TWA Flight 514, Boeing 727
On approach to Dulles International Airport in Washington, D.C., the flight was cleared for a non-precision approach and descended to an unsafe altitude while still 25 miles from the airport. Aligned with the extended centerline of the assigned runway, the flight struck Mt. Weather at an altitude of approximately 1,800 feet. The accident airplane was not equipped with GPWS, and, as a result of this accident, the FAA mandated the installation of GPWS on all commercial flights.
See accident module
December 20, 1995, American Airlines Flight 965, Boeing 757
While on approach to Cali, Colombia, the flight maneuvered away from the cleared approach path, apparently unsure of their location. During this maneuvering, the flight impacted high terrain in the vicinity of the airport. The airplane was equipped with GPWS, which functioned normally, but, due to the terrain profile, did not provide adequate warning to the crew. The investigation concluded that this accident was attributed to flight crew human error involving navigational and crew resource management lapses. This CFIT accident became the catalyst for requiring the installation of terrain awareness and warning systems in transport airplanes.
See accident module
Technical Related Lessons
CFIT accidents are often attributable to errors/lapses in human performance. A reduction in the rate of CFIT accidents can be achieved through the combination of proper flight deck human interface architecture, robust flight crew training programs, and additional airplane-based protection systems (e.g., GPWS) to mitigate the rare flight crew lapses. (Threat Category: Flight Deck Layout/Avionics Confusion)
- At the time of this accident in 1992, GPWS was standard equipment on most of the world's airline fleet. As a result of testing conducted by the French aviation authorities in the mid-1970's, GPWS was recommended for French air carriers, but was not specifically required. As a result, Air Inter had not equipped their fleet, including the A320, with GPWS. The French accident investigators concluded that, in the minutes prior to flight's impact into La Bloss Mountain, several human performance lapses may have occurred which precipitated the accident. It was further concluded by the investigators that, had GPWS been installed, it would have prevented the accident.
Flight crew communication and coordination, especially during critical, or high workload phases of flight such as preparation for takeoff or landing, should be aimed at achieving and maintaining proper situational awareness and airplane flight path and configuration control. (Threat Category: Crew Resource Management)
- As related in the accident report, flight crew communication and coordination did not indicate that effective crew resource management practices were employed. The accident report indicated that crew communication appeared to have been minimal, and cooperation between the pilots seemed strained. As a result, key factors related to autoflight system configuration and engagement status may have been missed, or not communicated. While it could not be conclusively determined by investigators, they believed that this lapse may have allowed an unintended autoflight mode to have been engaged and may have led to the Air Inter CFIT accident.
Common Theme Related Lessons
Once a safety technology or strategy is widely demonstrated and widely accepted to be highly effective in reducing risks in major safety areas, it is incumbent upon safety authorities to initiate the process which leads to the eventual implementation of that technology or strategy within the fleet under the jurisdiction of that authority. (Common Theme: Organizational Lapses)
- As a result of a number of CFIT accidents dating back to the 1960's, the installation of GPWS had been mandated by the majority of aviation authorities worldwide beginning in the mid-1970's. Based on separate research, French aviation authorities determined that while GPWS could aid in preventing accidents, based on concerns related to operational nuisance warnings, installation of GPWS was only recommended for the commercial aviation fleet within France. Based on the result of this research, Air Inter had elected not to install GPWS on its A320 fleet. The accident investigators concluded that if GPWS had been installed, it would have prevented the accident. Following the accident, operational regulations were adopted which required the installation of GPWS on essentially all of the French commercial airline fleet.