
Fokker 28

Copyright Trevor Ogle - used with permission
Air Ontario Flight 1363, C-FONF
Dryden, Ontario, Canada
March 10, 1989
Flight 1363, a Fokker 28 airplane operated by Air Ontario, departed Thunder Bay (Ontario) about one hour behind schedule, on a flight to Winnipeg, with an intermediate stop in Dryden.
During the stop in Dryden, heavy snow fell, covering, and freezing on the wings. Flight 1363 arrived from Winnipeg with an inoperative Auxiliary Power Unit (APU), and since the airport had no ground start equipment, the flight was required to keep one engine running during passenger loading/unloading. With an engine running, it was not possible to deice the airplane even though heavy snowfall existed at Dryden. At 12:09 local time, with ice accumulations on the wings, the airplane started its take-off roll using slush-covered runway 29. The pilot flying rotated the airplane at the prescribed speed, however, the airplane lifted off momentarily and then settled back onto the runway. Following a second rotation, the airplane lifted off at the 5,700-foot point of the 6,000-foot runway. No altitude was gained, and the aircraft settled in a nose-high attitude, striking trees. The aircraft crashed and came to rest in a wooded area approximately 3,200 feet past the departure end of the runway and caught fire. Both pilots, one flight attendant, and twenty-one passengers were killed. Forty-four passengers and one crew member survived with injuries.
The investigation commission concluded that the captain, "as the pilot-in-command, must bear responsibility for the decision to land and take off in Dryden on the day in question. However, it is equally clear that the air transportation system failed him by allowing him to be placed in a situation where he did not have all the necessary tools that should have supported him in making the proper decision."
On Friday March 10, 1989, the crew checked in at Winnipeg at approximately 0640 local time and were advised through dispatch that the Auxiliary Power Unit (APU) of the airplane scheduled for their flight was inoperative. Flight 1363 was the second part of the day's flying schedule which consisted of a Winnipeg to Thunder Bay round trip, with intermediate stops at Dryden.
It was the beginning of the March school break with many passengers having connecting flights in Winnipeg. At Thunder Bay the flight was refueled on the basis of a passenger load of 55. However, an additional 10 passengers were added, placing the aircraft over the computed maximum allowable gross weight for takeoff. After discussion over the course of action, the captain ordered a fuel offload and retained the extra passengers. Due to this delay, many passengers expressed concerns about their connecting flights. The flight subsequently departed for Dryden 64 minutes late. Following arrival in Dryden, ground servicing was conducted with an engine running, since there were no ground start facilities available, and the APU was inoperative. A turbine engine requires a source of high pressure air during the start sequence. This air can be supplied by a ground start unit, connected to the airplane while it is parked, or from the APU, which is installed on the airplane, and when running can supply both an air source, and auxiliary electrical power for the airplane. Since neither source was available, and engines typically need to be shut down for ground operations, the crew elected to leave one engine operating during the layover at Dryden. This allowed safe loading of passengers.
During the stop in Dryden, snow was falling and accumulating on the airplane. The first officer commented on the radio at 1200 CST, "...quite puffy snow, looks like its going to be a heavy one." Shortly after beginning to taxi, seeing snow and ice covering the wings, a passenger asked a flight attendant when the airplane was going to be de-iced. The flight attendants did not inform the flight crew of these expressed concerns about the need to de-ice.
The APU had been inoperative for five days prior to the crash, and the airplane had been dispatched under provisions of the Minimum Equipment List (MEL). This left the crew with a difficult decision at Dryden. If engines were shut down, the airplane would be effectively stranded at Dryden, as no ground start equipment was available for restart, and the APU was inoperative. Also, with an engine running, deicing would be prohibited due to associated hazards to the deicing ground crew from jet blast.
In order to continue the flight beyond Dryden, at least one engine needed to be left running, preventing the possibility of deicing. The captain finally elected not to de-ice.
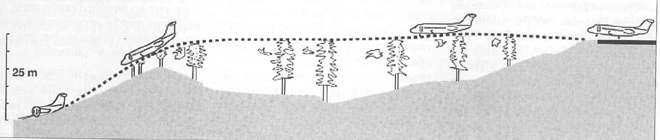
Once reaching the runway, takeoff was further delayed for approximately four minutes due to landing traffic. During that four-minute period, more snow accumulated on the airplane. At 1209 local time Flight 1363 started its takeoff roll. At the prescribed airspeed, the captain rotated the airplane. The airplane slowly lifted off, but due to wing contamination from snow and ice, sank back onto the runway. There was a second rotation and the airplane lifted off 100 meters away from the opposite end of the runway and crashed into trees off the end of the runway.
The aircraft was destroyed by impact and fire. Both pilots, one flight attendant, and twenty-one passengers were killed. Forty-four passengers and one crew member survived with injuries.

This photo with the broken trees shows the flight path the aircraft followed. The marks of the cut-off trees were used to reconstruct the flight path. By varying engineering parameters in an engineering simulation, the investigators verified that the airplane, with the observed amount of ice on its wings, could not have climbed away from the runway.
The Dryden accident was investigated by the Canadian government and documented in the report titled Commission of Inquiry into the Air Ontario Crash at Dryden, Ontario. The Commission concluded that the captain, "as the pilot-in-command, must bear responsibility for the decision to land and take off in Dryden on the day in question. However, it is equally clear that the air transportation system failed him by allowing him to be placed in a situation where he did not have all the necessary tools that should have supported him in making the proper decision."
The commission conducted an in-depth investigation of the entire Canadian air transportation system. Dozens of witnesses were interviewed; approximately 34000 pages of notes were taken; 177,000 pages of documentation were reviewed. The final report was made public in March 1992. It consists of 4 volumes, and approximately 1700 pages. The following issues were cited as relevant to the accident and were addressed in the accident report. A link to the entire accident report is provided here. (Commission of Inquiry Report - Volume I, Volume II, Volume III, Technical Appendices) Note: The report is quite large and may take some time to load.
The accident report is organized into nine parts, and relevant findings are distributed throughout each part:
Part 1 - Introduction
Part 2 - Facts Surrounding the Crash of Flight 1363
Part 3 - Crash, Firefighting, and Rescue Services
Part 4 - Aircraft Investigation Process and Analysis
Part 5 - The Air Carrier-Air Ontario, Inc.
Part 6 - Transport Canada
Part 7 - Human Factors
Part 8 - Legal and Other Issues Before the Commission
Part 9 - Consolidated Recommendations
General Appendices
The final accident report contains 191 recommendations on multiple topics. The 191 safety recommendations were mostly related to ground ice procedures, de-icing, de-icing fluids, training, etc. The consolidated recommendations are available beginning in Part 9 of the final report (Report Volume III).

Copyright Kevin Wachter - used with permission
The relevant regulations and associated discussions pertinent to this accident are contained in Volume III of the final accident report, beginning on page 1000.

Copyright Den Pascoe - used with permission
The investigators identified numerous cultural and organizational factors that were believed to be related to conditions in place leading up to this accident. A complete discussion of these factors is contained in Parts 5 (Volume II) and 6 (Volume III) of the final accident report.
- A take-off with ice on the wing surface, especially near the leading edge constitutes a hazardous condition.
- Airplane performance was predicated on the assumption that the airplane would be free of contamination.
Wing contamination can affect the lifting properties of a wing and can have catastrophic effects on field length required for takeoff, and the airplane's ability to climb after liftoff.

25 February 1969, Fokker 28 operated by LTU, registered PH-ZAA, Hanover, Germany
On 25 February 1969, the crew of an LTU F-28 aircraft attempted to take off from runway 09 left on a demonstration flight from Hanover Airport, Germany. At rotation speed, the captain rotated the aircraft to about 12°, and the aircraft lifted off. It immediately rolled to the right to a bank angle of about 25°, which could not be corrected by aileron control. The aircraft did not accelerate and descended until the right-wing tip struck the runway. The aircraft rolled to the left and then to the right, and the captain rejected the takeoff. The aircraft came to rest approximately 50 meters to the right of the runway and 1975 meters from where the takeoff roll had begun. The stick-shaker had activated three times while the aircraft was airborne. The only damage to the aircraft was to the right wing, the flap, and the aileron. None of the two crew or nine passengers was injured. It was determined that the accident was the result of ice contamination on the wing.
26 January 1976, Fokker 28 operated by Turkish Airlines registered TC-JAO, Izmir, Turkey
On 26 January 1976, the crew of a Turkish Airlines F-28 aircraft attempted to take off from Cumaovasi Airport, Izmir, Turkey. The aircraft became airborne after a ground roll of approximately 975 meters. However, when it was 8 to 10 meters above the ground, it yawed to the left and pitched nose down. The aircraft contacted the ground again and struck a drainage ditch, skidded, disintegrated and caught fire. Four crew members and 62 passengers died as a result of the accident; one crew member and 6 passengers survived. Investigators concluded that the wing had been contaminated with ice that had accumulated as frost the night before the accident. It was concluded that the probable cause of the accident was that the aircraft stalled because of over-rotation and frost accretion on the wings.
13 January 1982, Air Florida B-737-200, N62AF, Washington, D.C
Air Florida Flight 90 crashed shortly after takeoff from Washington National Airport, Washington, D.C. The Boeing Model 737-200 experienced difficulty in climbing immediately following rotation and subsequently stalled. The airplane struck the heavily occupied 14th Street Bridge connecting Arlington, Virginia with the District of Columbia, and then crashed into the ice-covered Potomac River. Seventy of the 74 passengers and four of the five crew aboard were killed along with four occupants of vehicles on the bridge. Loss of control was determined to be due to reduction in aerodynamic lift resulting from ice and snow that had accumulated on the airplane's wings during prolonged ground operation at National Airport. Contributing to the airplane's poor takeoff performance was a significant engine thrust shortfall believed to be due to anomalous engine thrust indications on both engines caused by engine pressure ratio (EPR) Pt2 probes which were believed to have been plugged with snow and ice during ground operation.
See accident module
15 November 1987, Continental Airlines DC 9-10, N626TX, Denver, Colorado
"Flight 1713 was cleared for a runway 35L take-off, 27 minutes after de-icing. On take-off, the DC-9 over rotated. The aircraft descended back, and the left wing struck the ground, causing it to separate from the fuselage. The left side of the cockpit and forward fuselage struck the ground next, and the aircraft continued to skid inverted. The investigation concluded that the accident was the result of ice contamination on the upper surface of the wing and a loss of control during rapid takeoff rotation by the first officer.
- As a result of the crash of Air Ontario Flight 1363, and the resulting investigation, many significant changes were made to the Canadian Air Safety regulations. These included not only new procedures regarding de-icing, but also many new regulations intended to improve the general safety of all future flights in Canada.
- Four air carrier Advisory Circulars were also issued by the Canadian government on the following subjects:
- Take-off during icing conditions
- Proposed new legislation regarding aircraft critical surface contamination & training
- Winter operations in ground icing conditions in Toronto
- Winter operations - new information on hold over times
- The Canadian Minister of Transport issued a letter encouraging the use of Type II deicing fluids.
- The Canadian Aviation Safety Board (CASB) initiated an investigation immediately after the March 10, 1989, Dryden crash. However, the Government of Canada replaced the CASB with an independent Commission of Inquiry on March 29, 1989. The Honorable Virgil P. Moshansky, was named as Commissioner, and was assigned the investigative responsibility of the Dryden accident, in place of the former CASB.
There were no FAA regulatory or policy changes resulting from this accident. However, the Air Florida 737 accident in Washington, D.C. in January 1982, was also the result of an attempted takeoff with wings contaminated by ice and snow and formed the basis for many winter weather requirements in place today within the United States. For a detailed listing of these regulatory changes, see the Air Florida accident module contained elsewhere in this library.
AD 94-25-03
This AD applicable to all Fokker Model F-28 series airplanes requires a revision to the Airplane Flight Manual (AFM) to prohibit takeoff in certain icing conditions unless either a tactile inspection is performed, or specific takeoff procedures are followed.
This amendment supersedes AD 94-25-27 by adding a requirement for certain airplanes, for modification of the wing leading edge ice protection system to include on-ground wing ice protection, and a new revision to the AFM.
Airplane Life Cycle:
- Operational
Accident Threat Categories:
- Inclement Weather / Icing
- Crew Resource Management
- Landing / Takeoff Excursions
Groupings:
- Loss of Control
Accident Common Themes:
- Organizational Lapses
- Human Error
Organizational Lapses
Air Ontario dispatched Flight 1363 with the APU inoperative. APU inoperative dispatch is allowed per the MEL, however, at Dryden, no equipment was available to restart engines if they were shut down. This required that during the ground time at Dryden, one engine be kept running. This prevented deicing prior to takeoff from Dryden and led to a takeoff attempt with accumulated snow on the wings. The organizational lapse that dispatched the flight in an MEL configuration, to an airport that could not accommodate the MEL configuration, placed the flight crew in a situation without the necessary tools for proper decision making.
Human Error
The flight crew made the decision to depart Dryden without deicing the airplane, even though snow had accumulated on the wings. Airplane performance is predicated upon the wings being free of contamination. The accumulation of snow had an adverse effect on the wing's ability to produce lift, and for the airplane to lift off and climb.

22 March 1992, USAir Fokker 28, N485US, La Guardia Airport, New York, New York
On 22 March 1992, a Fokker 28 registration number N485US, USAir flight 405, crashed shortly after take-off from runway 13 at La Guardia Airport (New York). Twenty-four people survived, out of fifty-one passengers and crew. The airplane took off following deicing with type I deicing fluid, which at the takeoff temperature of 30 degrees, had an effective action period of approximately 15 minutes. The airplane had been deiced twice and took off 35 minutes after the second deicing. Following a rotation approximately 5 knots lower than the prescribed speed, the airplane lifted off, stalled, and crashed near the edge of a bay near the airport boundary. The investigators concluded that the wings had been contaminated by snow and ice prior to takeoff.
5 March 1993, Palair Fokker 100, PH-KXL, Skopje, Yugoslavia

On 5 March 1993, the Fokker 100 registered PH-KXL, Palair flight PMK 301, crashed shortly after take-off from runway 34 at Skopje Airport (Former Yugoslav Republic of Macedonia). Of the 97 people on board, fourteen people, including one crew member, survived. The meteorological conditions were wind 350°/5kt, moderate snow, external temperature 0°C, dew point temperature -1°C. The investigation showed that the wing had stalled at an angle of ten degrees. The airplane had suffered a sudden roll followed by roll oscillations, which the crew had been unable to control. It was concluded by the investigators that the wings had been contaminated with snow and ice prior to takeoff.
17 February 1991, Ryan International Airlines DC-9, N965PC, Cleveland, Ohio
Ryan Flight 590 landed at Cleveland at 23:44 and taxied to the mail ramp. Snow (dry and blowing) fell throughout the 35 minutes that the DC-9 was on the ground. Deicing service was not requested during this period. The aircraft stalled during takeoff and crashed, coming to rest 6500 feet from the runway threshold. The investigation concluded that the wings had been contaminated by ice prior to takeoff.

25 January 2007, Régional CAE Fokker 100, F-GMPG, Pau, France
During takeoff from Pau, the airplane lifted off and immediately rolled left and began to descend. The crew attempted to land, and the airplane contacted the ground near the end of the takeoff runway. The airplane collided with the airport perimeter fence, and a truck, before coming to rest in a field. The accident investigation concluded that the airplane stalled after takeoff due to ice contamination on the wings.
Technical Related Lessons:
Even small amounts of frost, ice, or snow can have catastrophic effects on airplane performance. (Threat Category: Inclement Weather/Icing)
- In this accident, a takeoff was attempted with wings contaminated by ice and snow. Small amounts of wing contamination can have profound adverse affects on the lifting properties of a wing. As a result, the ability of flight 1363 to develop sufficient lift to take off within the available runway length was inhibited. An unplanned delay in Dryden exposed the airplane to a snow accumulation on the wings that, due to the very cold fuel in the wings, subsequently formed ice, and degraded the wing's capability to generate lift. Takeoff performance can also be adversely impacted by an accumulation of slush on the runway which affects the acceleration characteristics of the airplane and increases the required field length.
Flight crew communications regarding airplane safety readiness should be open and effective. Each crewmember must clearly give and receive communication in such a way that the flight safety decisions represent the best product of this open, two-way communication. (Threat Category: Crew Resource Management)
- In this accident, passengers had questioned the cabin crew about snow accumulations on the wings; however, these questions were not passed on the flight crew. Air Ontario procedures at the time discouraged communication between flight and cabin crew members regarding operational issues, which are typically considered just the purview of the flight crew. Relaying questions from the passenger cabin would have been considered outside the scope of cabin crew duties and was therefore not conducted. In a fully functional crew resource management (CRM) environment safety related information from passengers or other crew members should not be discouraged, as cabin crew members are considered to be a CRM resource, and within operational protocols (such as communicating during takeoff roll,) should be expected to identify a potential safety issue to the flight crew.
Common Theme Related Lessons:
Organizational processes should strive to minimize placing an individual or crew in a position of making safety decisions over conflicting priorities, and inadvertently initiating a safety lapse. (Common Theme: Human Error)
- Flight 1363 was dispatched into a situation that left the flight crew with the decision to either attempt a takeoff with an airplane that had not been deiced during snow/ice conditions, or cancel the flight in Dryden, inconveniencing many passengers. This dilemma should have been anticipated earlier, and the proper safety decision made by organizational processes, rather than later placing the flight crew in a difficult situation at Dryden.